GENERAL INFORMATION
Synovial sarcoma is a common soft tissue malignancy accounting for 5 – 10 % of soft tissue sarcomas. Patients with synovial cell sarcoma are often between the ages of 15 and 35 years old; generally younger than patients with other types of soft tissue sarcomas. The most probable cellular origin is an undifferentiated mesenchymal cell. The tumor may be monophasic or biphasic meaning having one or two different types of cells that make up the tumor. The monophasic type is frequently composed of relatively uniform malignant appearing spindle cells with a fascicular arrangement. The biphasic type is similar to the monophasic but with epithelial clusters or glandular-like spaces. Synovial sarcoma has a fusion gene, SYT-SSX, which is the result of a chromosomal translocation unique for this tumor, t(x;18)(p11;q11), which is present in up to 90% of cases. Synovial sarcoma whether monophasic or biphasic stains positive for vimentin and epithelial makers such as cytokeratin and epithelial membrane antigen (EMA)
CLINICAL DATA
Third most common soft tissue sarcoma; 6-10%
Most commonly affects young adults aged between 15 and 35 years
Equal male and female prevalence
Occurs most often in paraarticular regions and not in the actual joints.
It can arise from tendon sheaths, bursae or joints capsules.
Most common soft tissue sarcoma of the foot and ankle
DIFFERENTIAL DIAGNOSIS
Biphasic synovial sarcoma
Malignant peripheral nerve sheath tumor
Carcinoma
Diffuse type tenosynovial giant cell tumor / PVNS
Poorly differentiated Synovial sarcoma
Malignant peripheral nerve sheat tumor
Fibrosarcoma
Hemangiopericytoma
Primitive peripheral neuroectodermal tumor
Monophasic synovial sarcoma
Fibrosarcoma
Leiomyosarcoma
Epithelioid sarcoma
Clear cell sarcoma
Palmar or plantar fibromatosis
CLINICAL PRESENTATIONS
Signs/Symptoms
Slow growing, palpable and often painful mass.
Symptoms may be present from days to as long as 20 years before initial diagnosis
Prevalence
Equal prevalence male and female
Age
Range 15 - 35 years old
Generally presents in a younger age than other soft tissue sarcomas
Sites
Most synovial sarcomas occur in the extremities (80%).
Predilection for lower limbs 60 – 70 %
Popliteal fossa being the most common location.
Most common soft tissue malignancy of the foot and ankle in patients between 6 and 35 years old.
Most of them are intermuscular in location and found within 5 cm of a joint.
Intra-articular origin is found in less than 10 % of the cases.
It can invade adjacent bone
May metastasize to regional lymph nodes
RADIOGRAPHIC PRESENTATION
X-rays
Normal in approximately 50% of the cases.
Soft tissue density with mineralization in 30% of cases. This type of mineralization usually presents as calcifications with an irregular contour often in a peripheral distribution.
In 11% to 20% of cases there may be a periosteal reaction, adjacent bony erosion or bone invasion.
 Plain Radiograph Synovial Sarcoma of Wrist Area with Calcifications
Plain Radiograph Synovial Sarcoma of Wrist Area with Calcifications
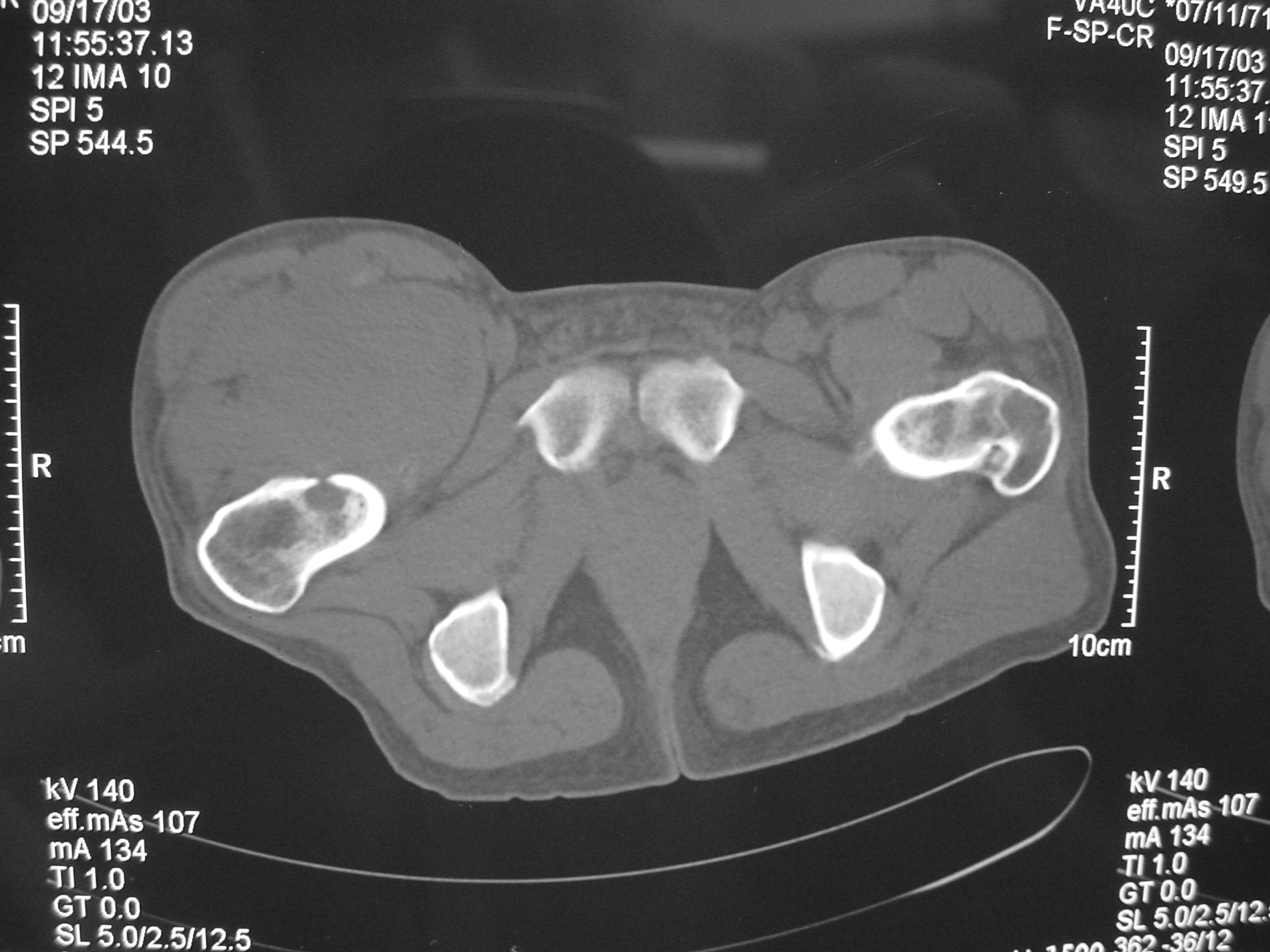 CT Scan Synovial Sarcoma of Thigh Invading Proximal Femur
CT Scan Synovial Sarcoma of Thigh Invading Proximal Femur
MRI
Shows multiloculated, heterogeneous mass.
“Triple Signal Intensity sign”; hypointense, isointense and hyperintense with fat on T2 – weighted MRI imaging. This sign is present in 30 to 50% of the cases. (Fig.3)
Under contrast enhancement Synovial Sarcoma appears heterogeneous and demonstrate areas of nodular enhancement.
In approximately 30% of cases a multiple vascular cannel may be identified
Synovial sarcomas may have a cystic appearance and are often mistaken for ganglion cysts especially those adjacent to tendons and in the foot and ankle.
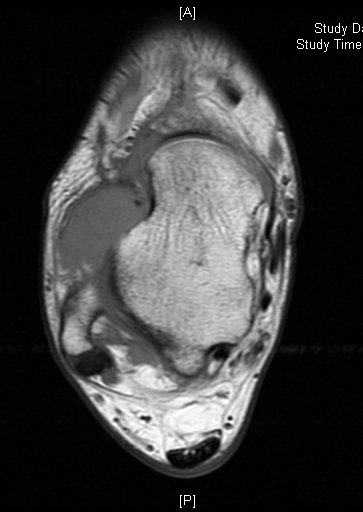 Fig. 1A MRI Axial T1 Synovial Sarcoma of Ankle
Fig. 1A MRI Axial T1 Synovial Sarcoma of Ankle
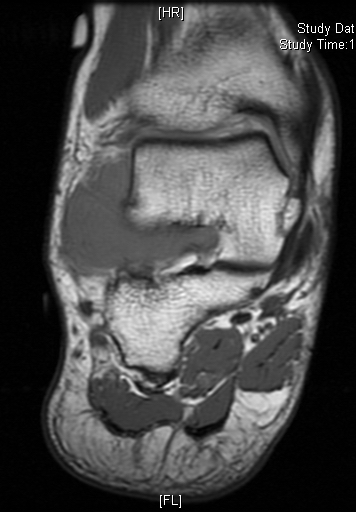 Fig. 1B MRI Cor T1 Synovial Sarcoma of Ankle
Fig. 1B MRI Cor T1 Synovial Sarcoma of Ankle
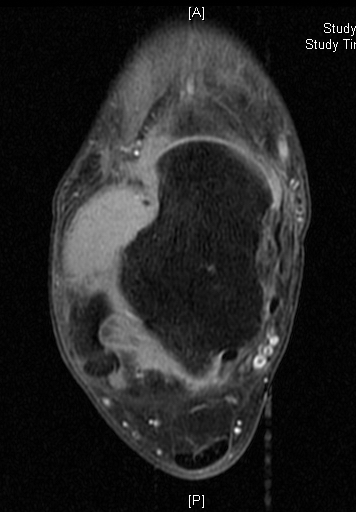 Fig. 1C MRI Ax T1 FS with Gadolinium - Synovial Sarcoma of Ankle
Fig. 1C MRI Ax T1 FS with Gadolinium - Synovial Sarcoma of Ankle
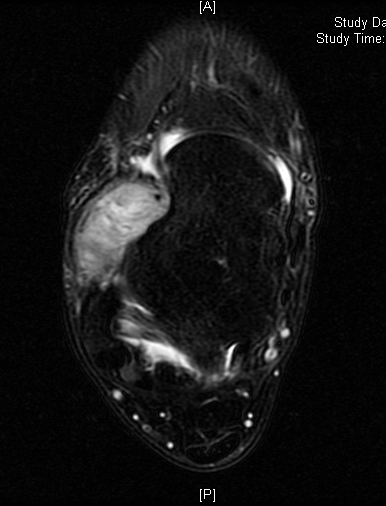 Fig. 1D MRI Ax T2 Synovial Sarcoma of Ankle
Fig. 1D MRI Ax T2 Synovial Sarcoma of Ankle
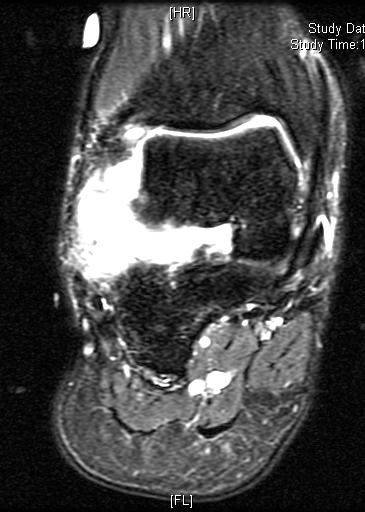 Fig. 1E MRI Cor T2 Fat Saturation - Synovial Sarcoma of Ankle
Fig. 1E MRI Cor T2 Fat Saturation - Synovial Sarcoma of Ankle
 Fig. 1F MRI Sag T2 FS Synovial Sarcoma of Ankle
Fig. 1F MRI Sag T2 FS Synovial Sarcoma of Ankle
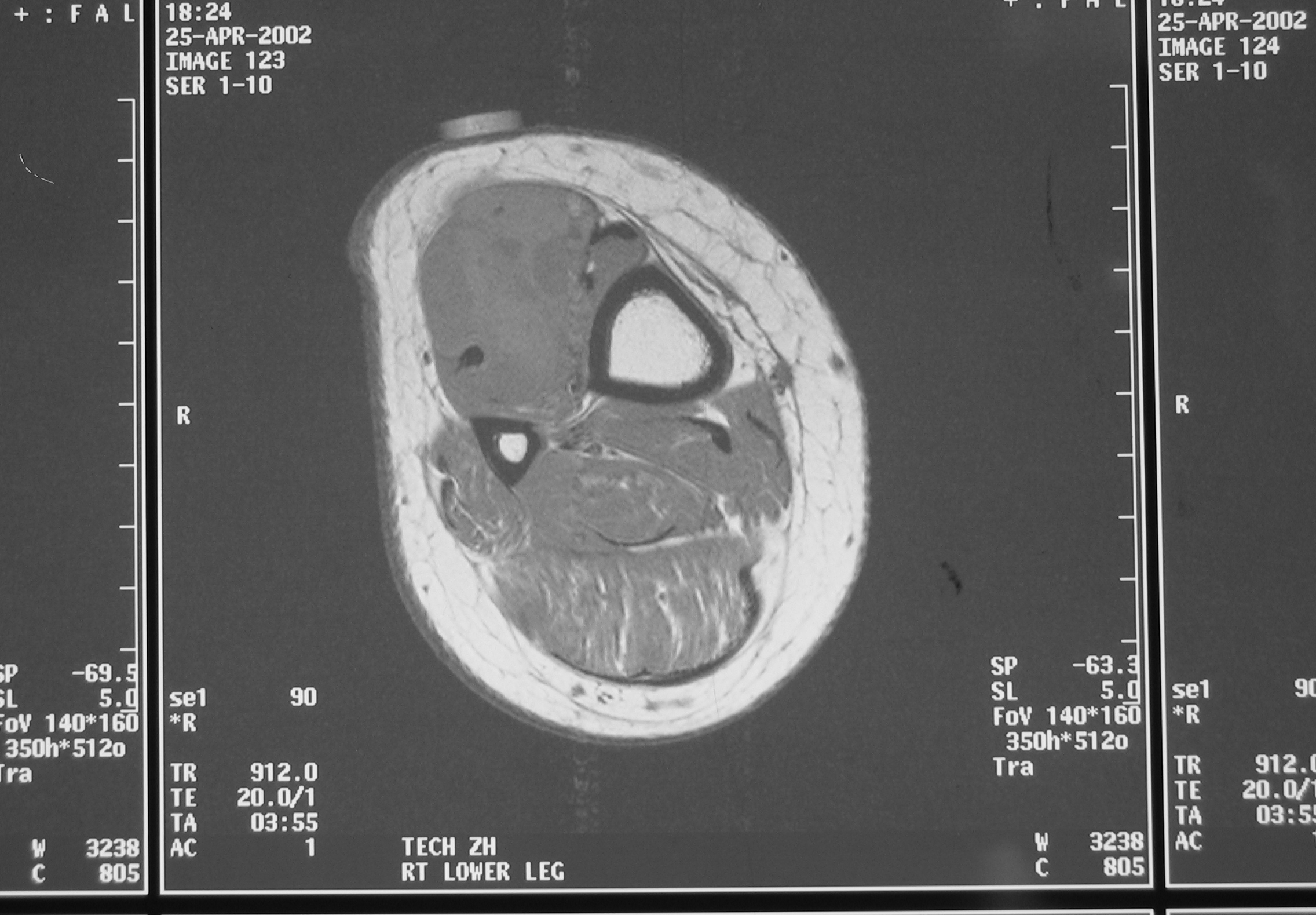 Fig. 2 MRI T1 Synovial Sarcoma of Leg
Fig. 2 MRI T1 Synovial Sarcoma of Leg
 Fig. 2A MRI T1 Synovial Sarcoma of Leg
Fig. 2A MRI T1 Synovial Sarcoma of Leg
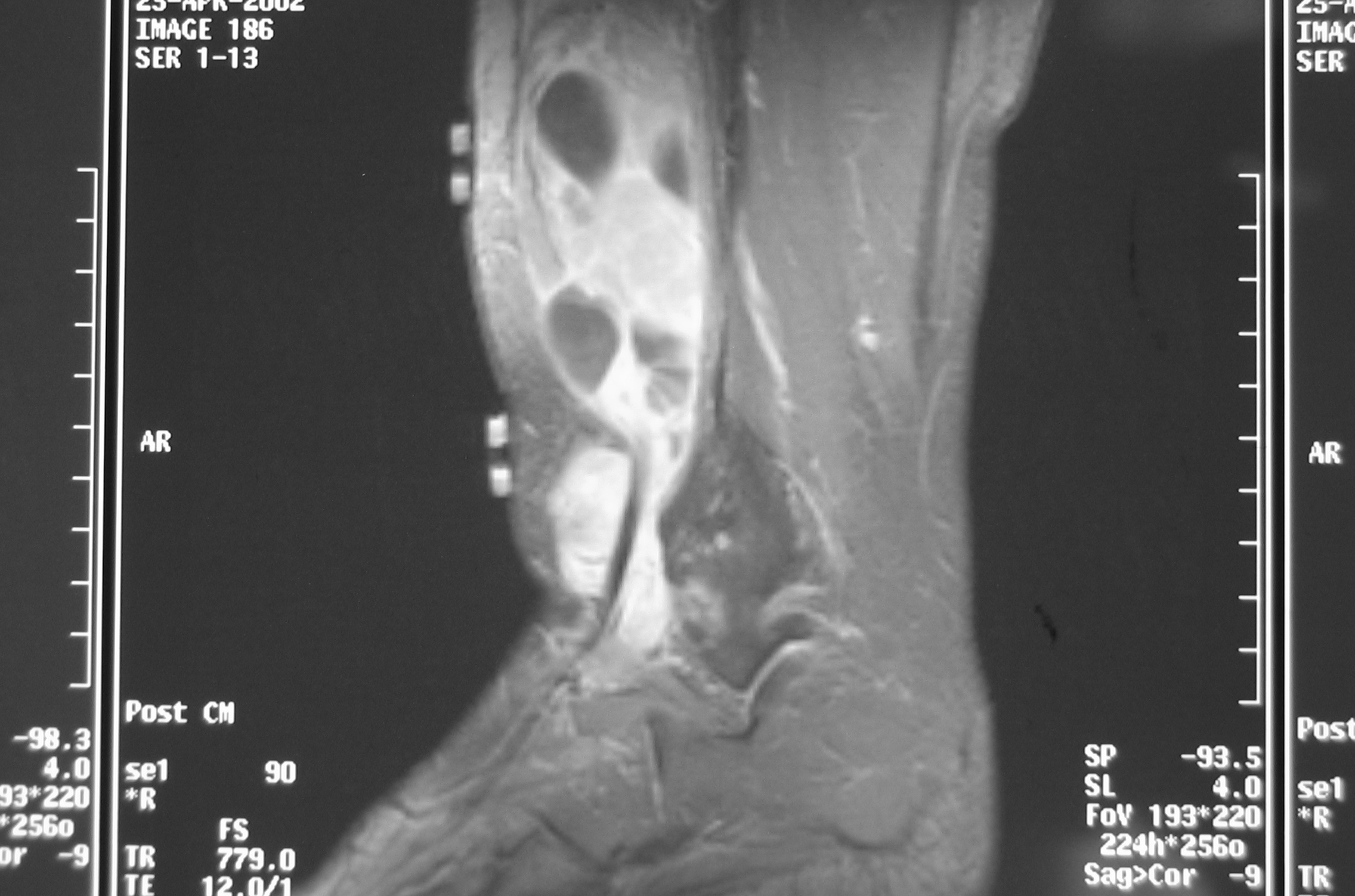 Fig. 2B MRI Sagittal T2 Synovial Sarcoma of Leg
Fig. 2B MRI Sagittal T2 Synovial Sarcoma of Leg
 Fig. 2C MRI Axial Synovial Sarcoma of Leg
Fig. 2C MRI Axial Synovial Sarcoma of Leg
 Fig. 3A MRI Coronal Synovial Sarcoma of Distal Thigh Knee Area
Fig. 3A MRI Coronal Synovial Sarcoma of Distal Thigh Knee Area
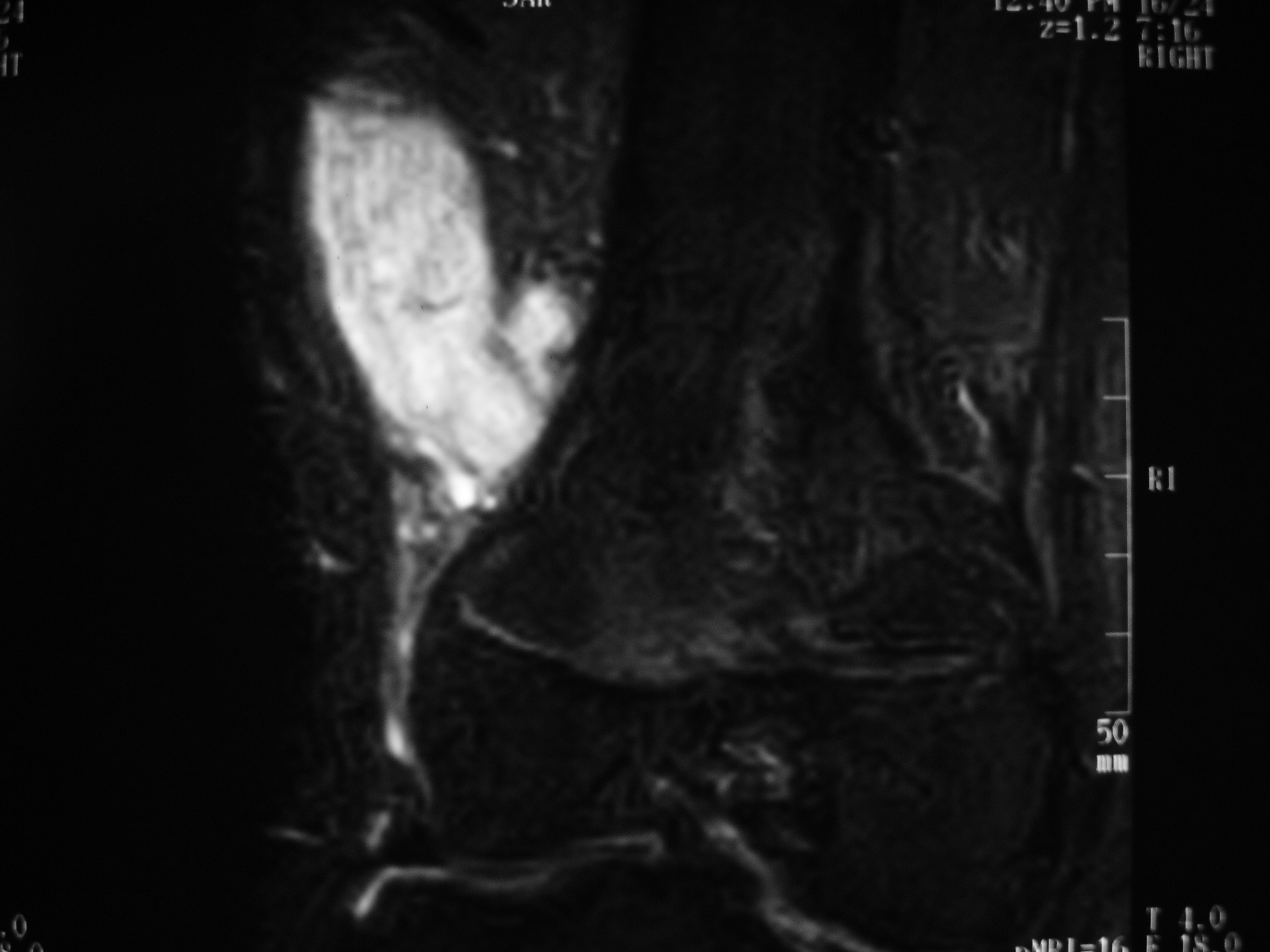 Fig. 3B MRI T2 Synovial Sarcoma of Distal Thigh
Fig. 3B MRI T2 Synovial Sarcoma of Distal Thigh
 Fig. 3C MRI Axial Synovial Sarcoma of Distal Thigh
Fig. 3C MRI Axial Synovial Sarcoma of Distal Thigh
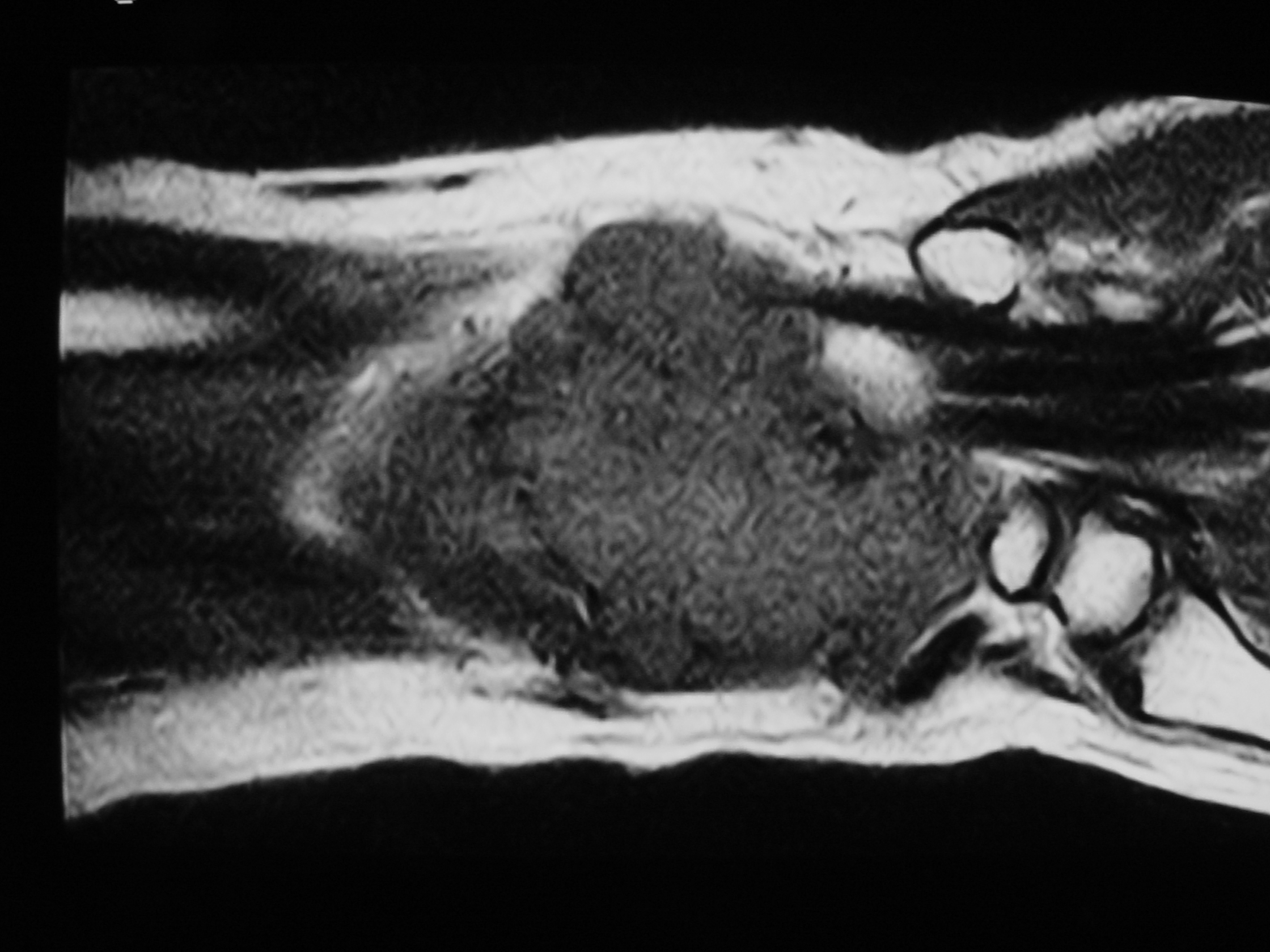 Fig. 5B MRI of Synovial Sarcoma of Wrist Area
Fig. 5B MRI of Synovial Sarcoma of Wrist Area
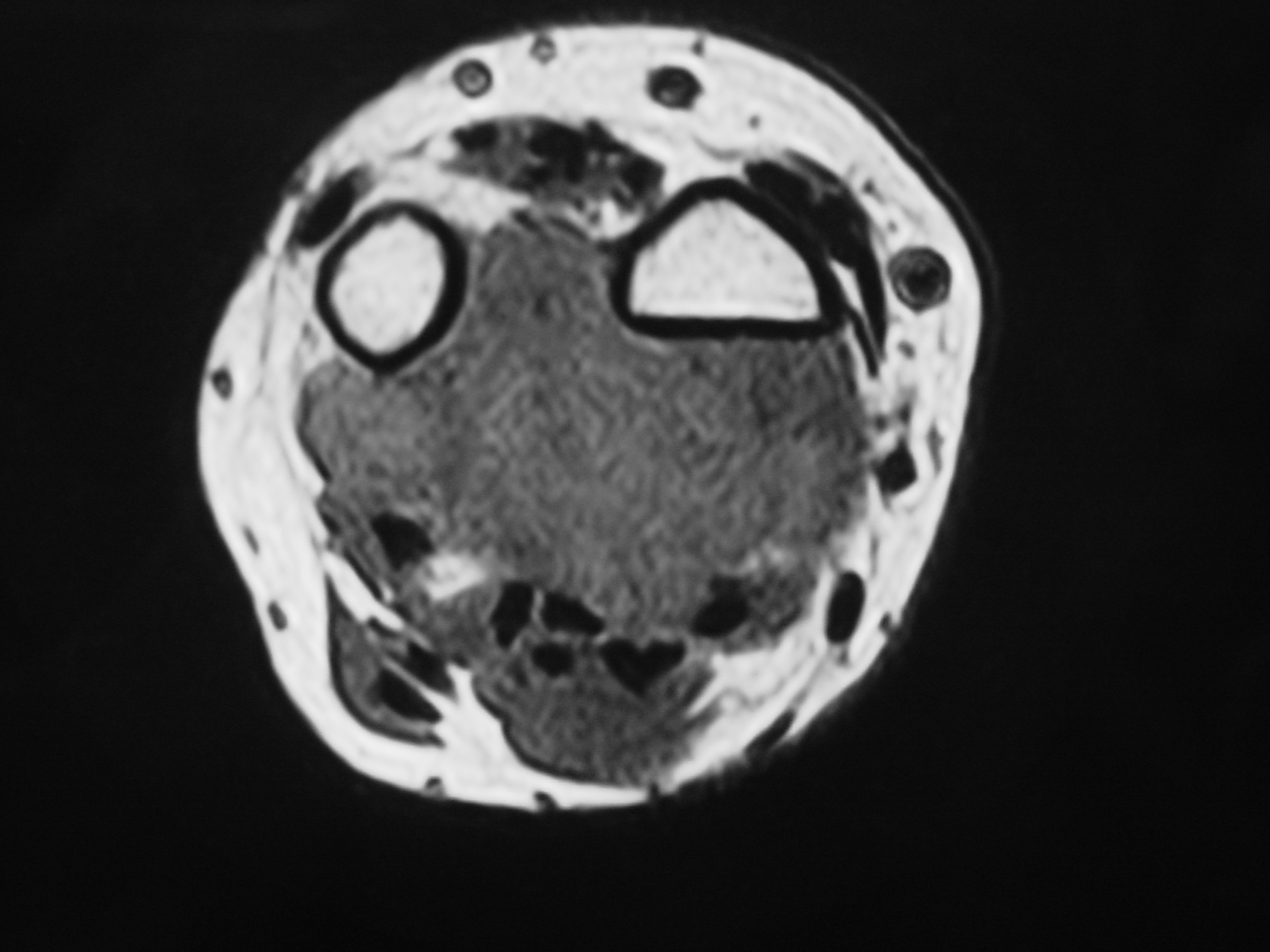 Fig. 5C MRI Axial T1 Synovial Sarcoma of Wrist Area
Fig. 5C MRI Axial T1 Synovial Sarcoma of Wrist Area
PATHOLOGY
Gross Pathology
Synovial sarcomas are usually circumscribed, round or multilobular masses
They may grow to >15 cm, but on average measure 3 to 5 cm in greatest diameter since many occur in the foot and ankle
Can be described as yellow to gray-white
The less differentiated variants often grow more rapidly and tend to be poorly circumscribed, with multiple areas of hemorrhage, necrosis, and cystic formation
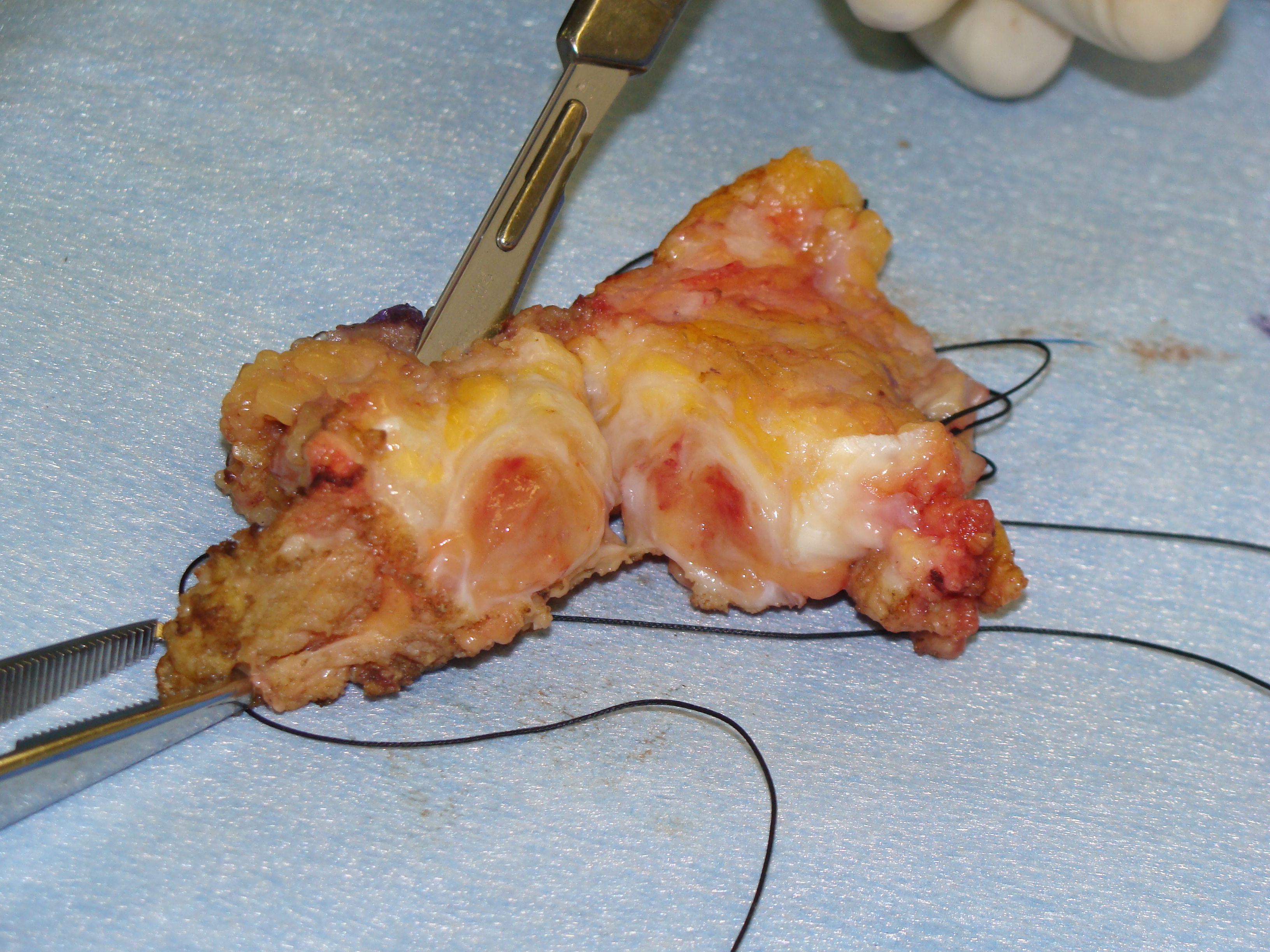 Fig. 6 Gross Specimen Synovial Sarcoma of Wrist Area
Fig. 6 Gross Specimen Synovial Sarcoma of Wrist Area
Microscopic Pathology
Synovial Sarcoma is composed of two different cell types
Spindle cell (small, uniform, and ovoid cells with pale nuclei and the cytoplasm is sparse)
Epitheloid cell (ovoid nuclei and abundant cytoplasm)
Biphasic form is composed of both epithelial-cell and spindle-cell components in equal proportions (Fig. 6-8)
Monophasic Fibrous type predominantly spindle cell.
Monophasic Epithelial type is difficult to differentiate from adenocarcinoma without cytogenetics and immunohistochemistry.
Poorly differentiated type demonstrates features of high grade small round cell tumor with dense cellularity, numerous mitotic figures, and areas of necrosis.
Inmunohistochemical profile: Vimentin (+), Cytokeratin (+), Epithelial Membrane Antigen EMA (+)
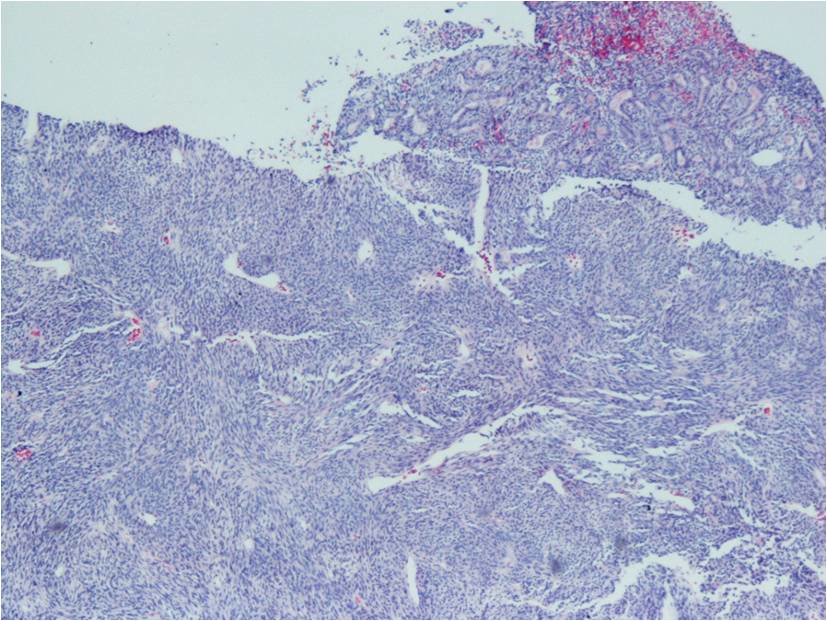 Fig. 7A Microscopic Pathology Intermediate Magnification Synovial Sarcoma of Ankle
Fig. 7A Microscopic Pathology Intermediate Magnification Synovial Sarcoma of Ankle
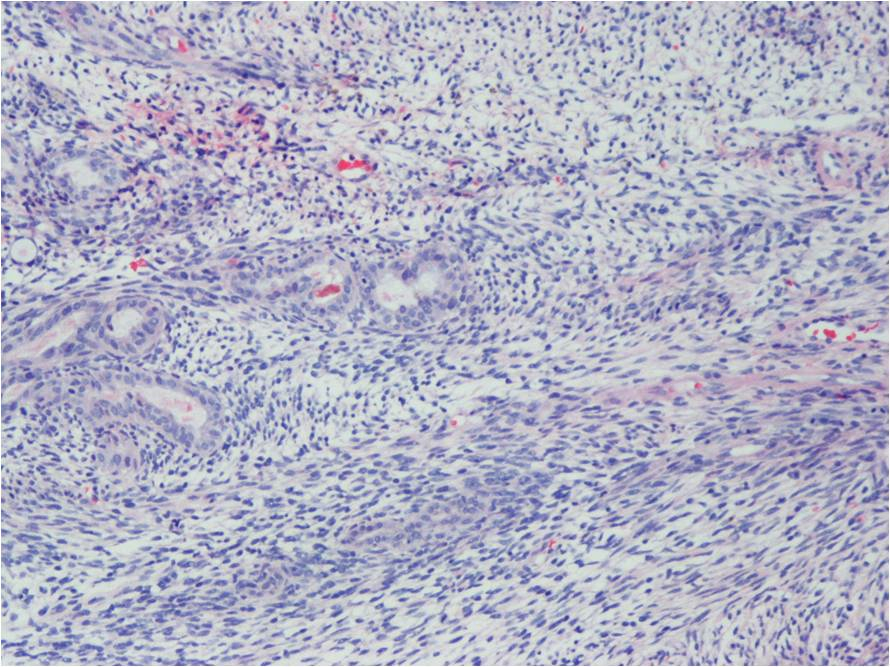 Fig. 7B Microscopic Pathology Intermediate Magnification Synovial Sarcoma
Fig. 7B Microscopic Pathology Intermediate Magnification Synovial Sarcoma
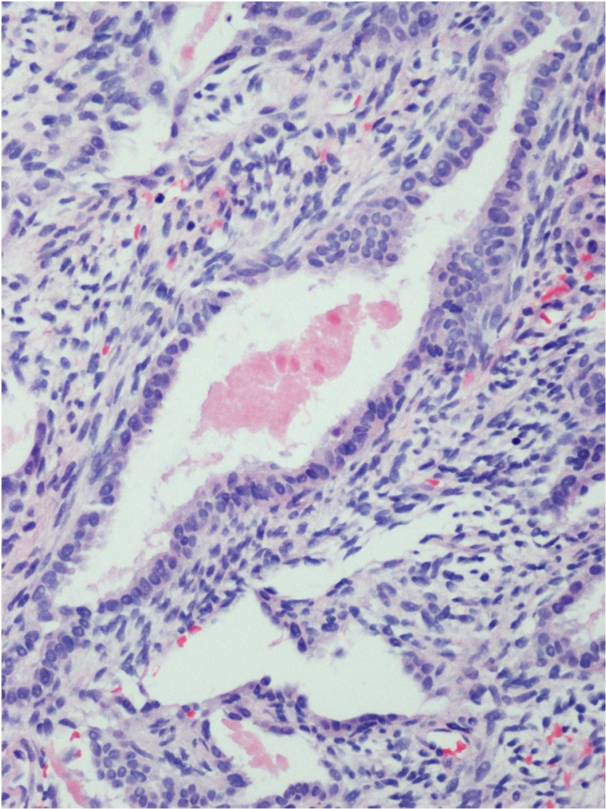 Fig. 7C Microscopic Pathology High Magnification Bipasic Synovial Sarcoma of Ankle
Fig. 7C Microscopic Pathology High Magnification Bipasic Synovial Sarcoma of Ankle
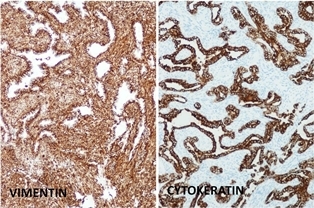 Fig. 7D Microscopic Pathology Immunohistochemical staining synoval sarcoma classic bipasic variety
Fig. 7D Microscopic Pathology Immunohistochemical staining synoval sarcoma classic bipasic variety
TREATMENT
Wide surgical excision is the mainstay of treatment for Synovial Sarcoma
High grade tumors:
Often requires either radical resection or wide surgical excision plus Radiotherapy
Amputation may be required for unresectable tumors
Tumors that are greater than 8 cm in diameter may be considered for administering Chemotherapy and Radiotherapy
Radiotherapy may improve local control
Chemotherapy is most often used when there is metastatic disease
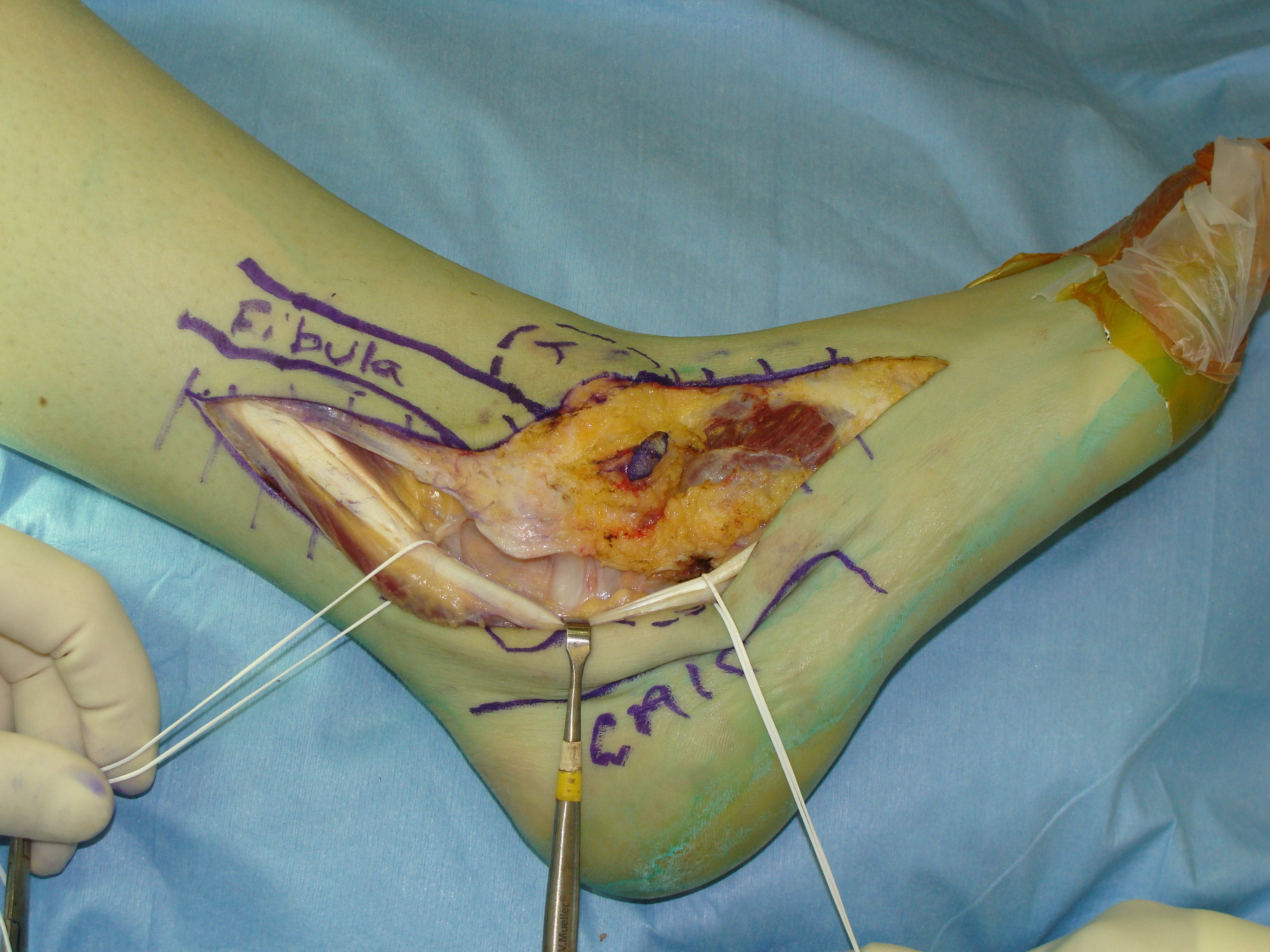 Fig. 8A Intraoperative Photo Synovial Sarcoma of Ankle
Fig. 8A Intraoperative Photo Synovial Sarcoma of Ankle
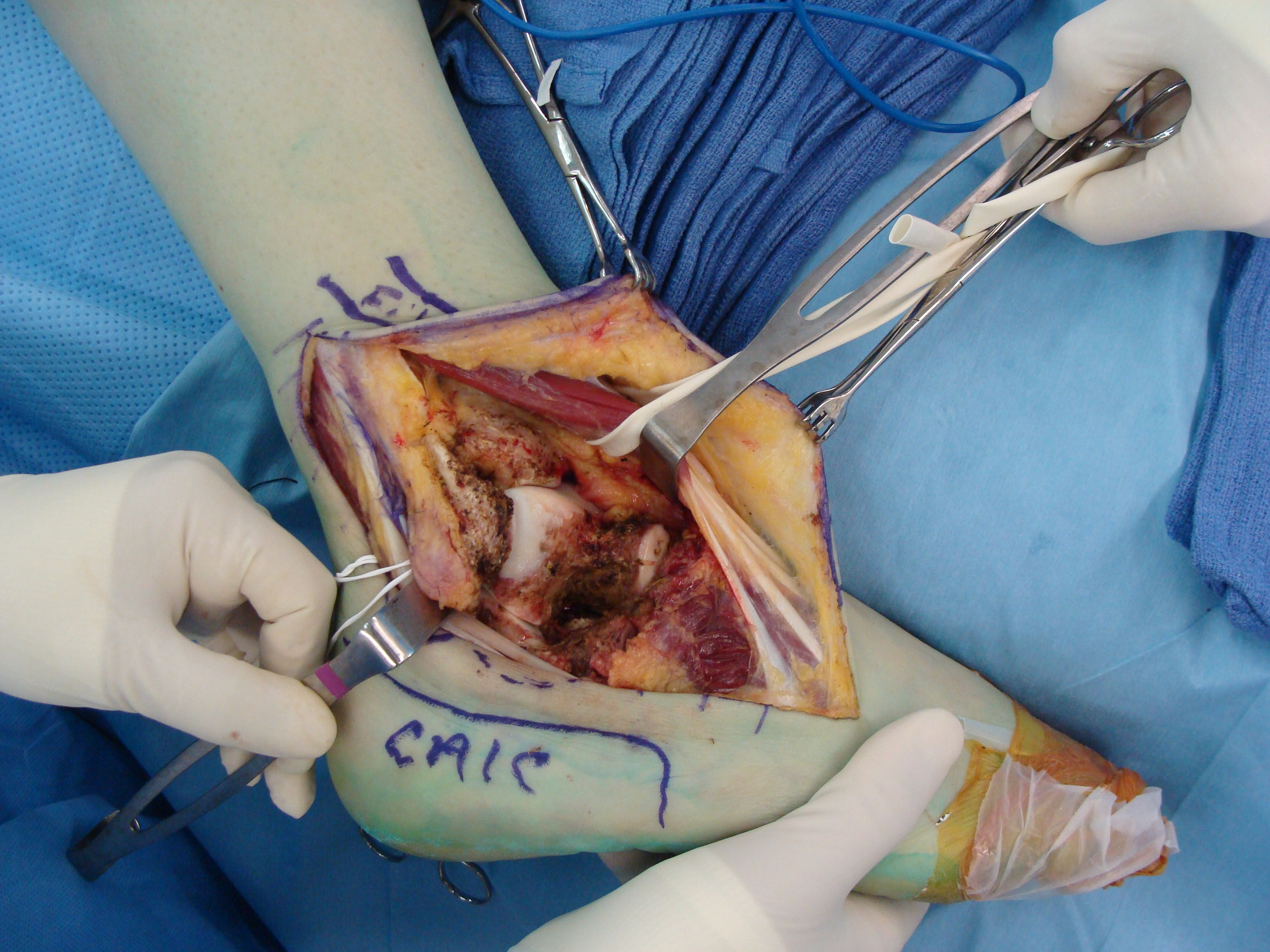 Fig. 8B Intraoperative Photograph after Resection of a Synovial Sarcoma from Ankle
Fig. 8B Intraoperative Photograph after Resection of a Synovial Sarcoma from Ankle
PROGNOSIS
5 year survival rates vary significantly, ranging from 36 to 76%
Large tumor size (> 5 cms), presence of bone or neurovascular invasion were found to be associated with the development of distant metastasis and decreased disease specific survival (mortality).
Patients with tumors that present with more than 20% of poorly differentiated patterns have the worse prognosis
50% of the patients with Synovial Sarcoma develop metastases.
Other prognostic factors have been correlated with an increase in the local recurrence rate including; proximal location of the tumor or positive margin after resection.
