GENERAL INFORMATION
Solitary fibrous tumor is a rare and usually benign mesenchymal tumor, composed of thick collagen and characteristically has a prominent haemangiopericytoma-like branching vascular pattern. Solitary fibrous tumors usually affect adult group (median age 50) and have no sex predilection. Occasional cases occur in children and adolescents. This entity has a broad site of distribution, arising from any soft tissue/visceral location. Close to 40% of the tumors are localized in the subcutaneous tissues. Painless and slow growth are the main sign/symptoms. Solitary fibrous tumor can also cause hypoglycemia due to insuline-like growth factor production (called paraneoplastic hypoglycemia), or local compression symptoms in case of large tumor (nasal cavity, the orbit and meninges). Malignant types may be infiltrative and metastasize (15-20%). Poor prognostic factors could be defined based on size of the tumor (˃ 10 cm), number of mitosis (˃ 4 mitosis/10hpf), atypia and positive margin after the resection. Grossly the masses are usually well circumscribed, white firm and partially encapsulated (Fig. 1-6); Necrosis and infiltrative margins may be present and are associated with aggressive behavior or malignancy. Microscopically these tumors show areas of hypercellularity mixed with hypocellular areas separated by collagen and haemangiopericytoma-like vessels. Spindle cells with minimal cytoplasm and elongated nuclei; Myxoid changes and multinucleated giant cells may be present. Immunohistochemical stains may show CD 34 (90-95%), CD99 (70%), BCL2, EMA and actin are positive. Complete excision is the treatment (Fig. 7-10).
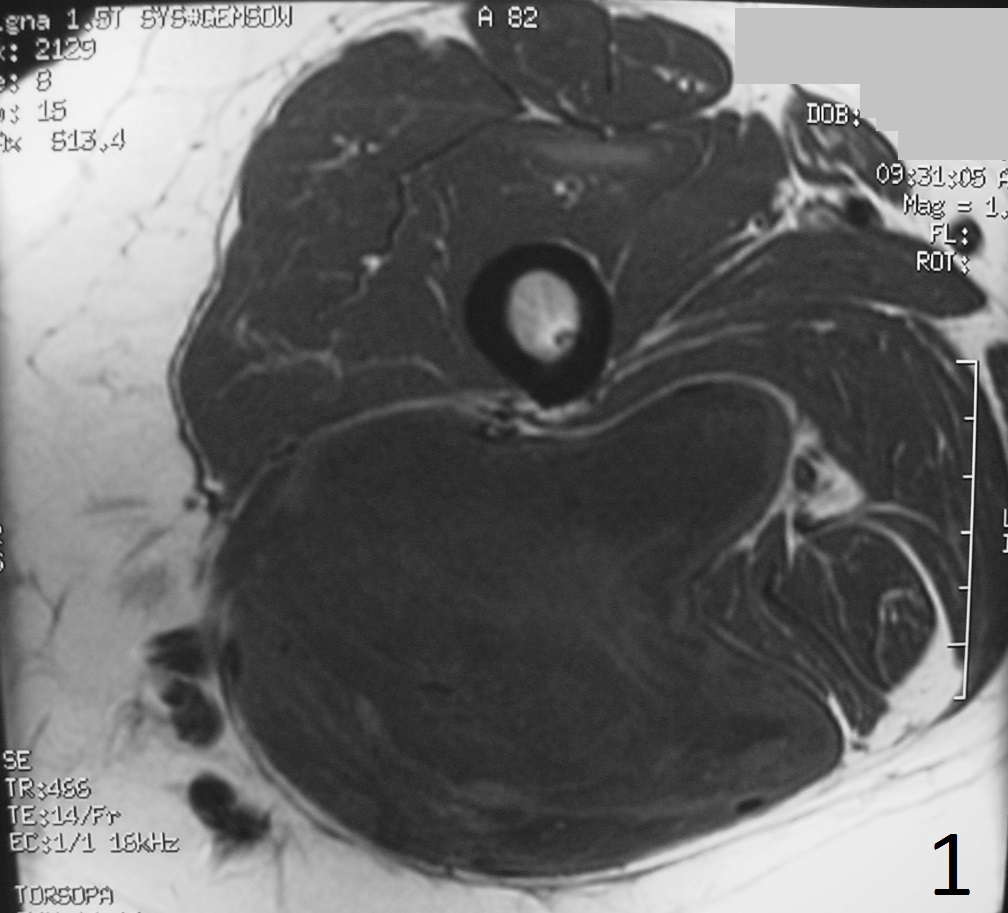 Fig. 1
Fig. 1
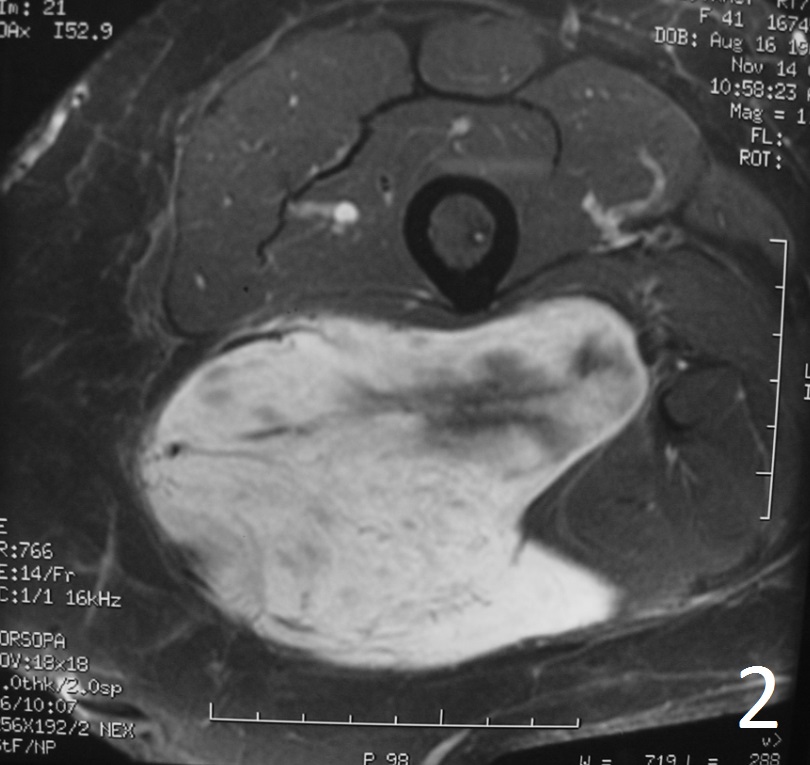
Fig. 2
Fig. 1-2: The MRI of a solitary fibrous tumor is non specific. Any type of sarcoma can appear similar. Axial MRI of the thigh shows a well circumscribed and big lobulated mass low/intermediate signal on T1W (Fig. 1), enhancement on T1W FS post-gadolinium images with some areas of necrosis (Fig. 2).
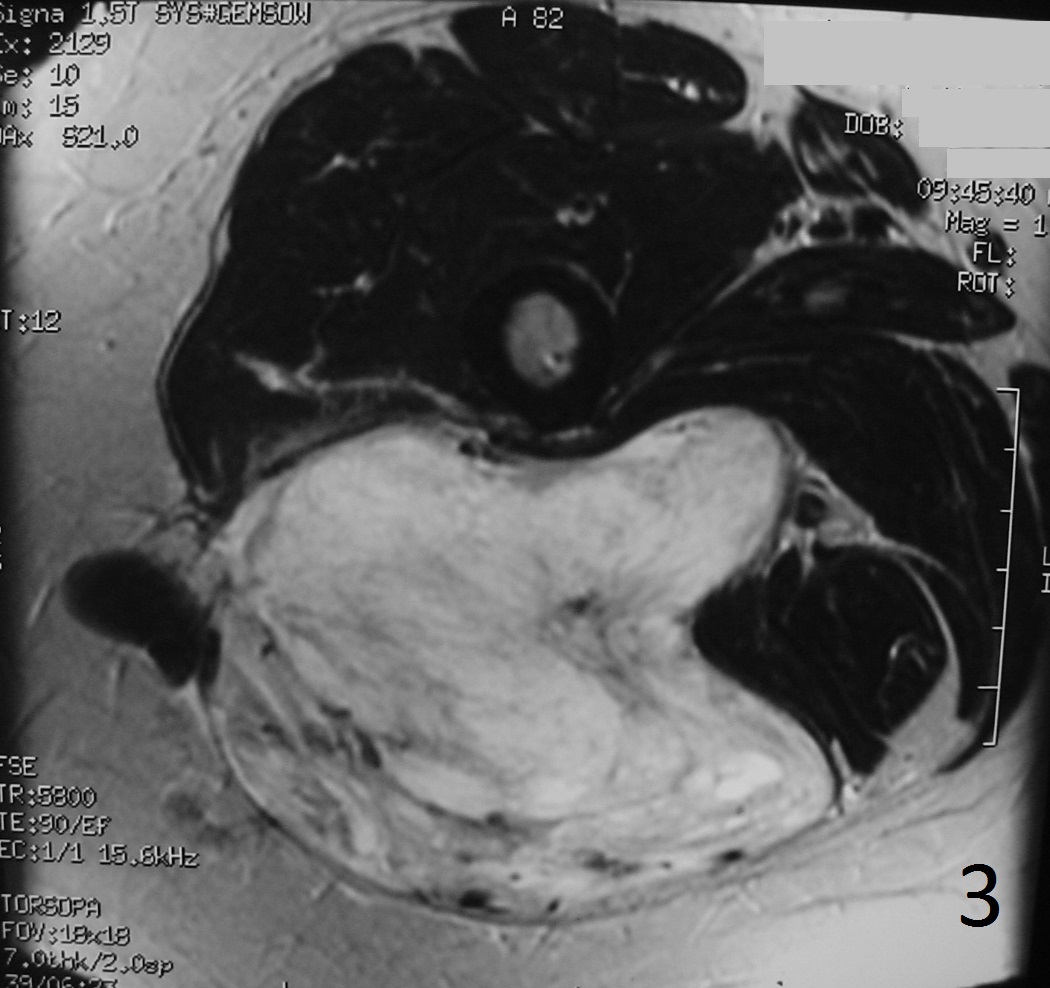
Fig. 3: Axial T2W image shows a mass with primarily high signal intensity although heterogeneous and heavily septated
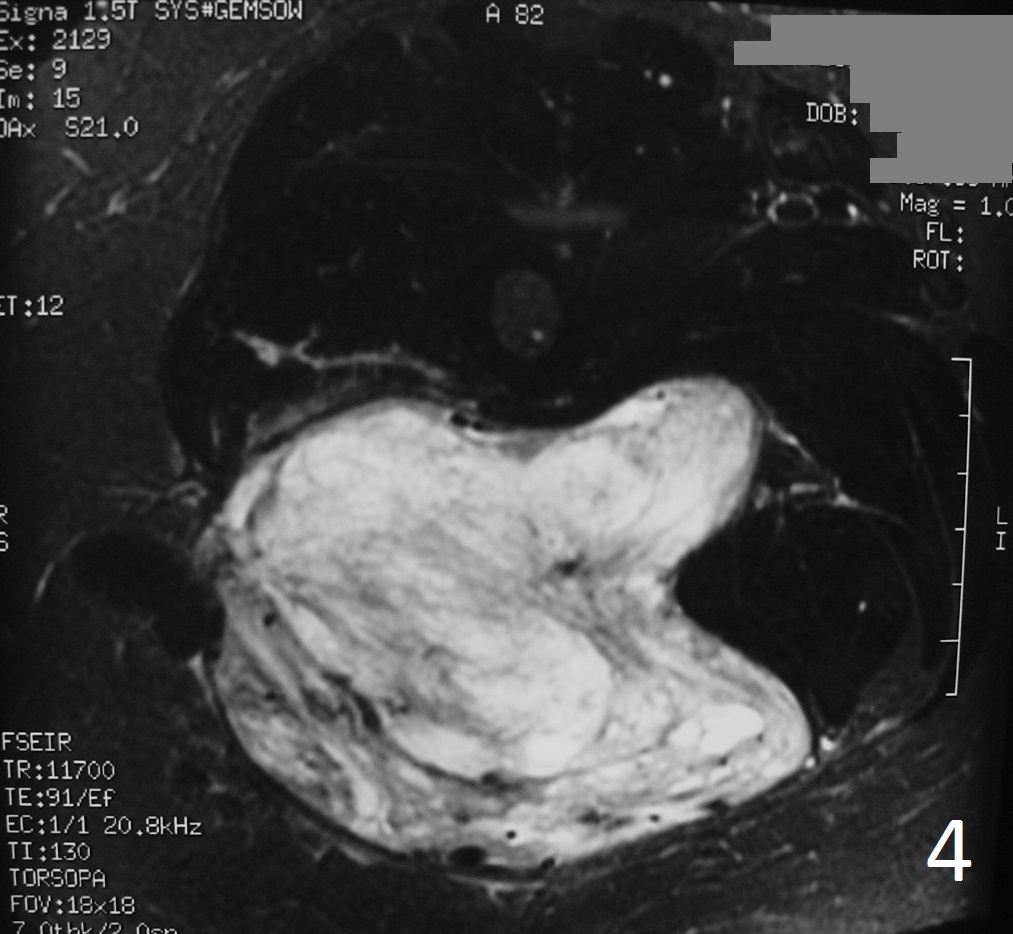
Fig. 4
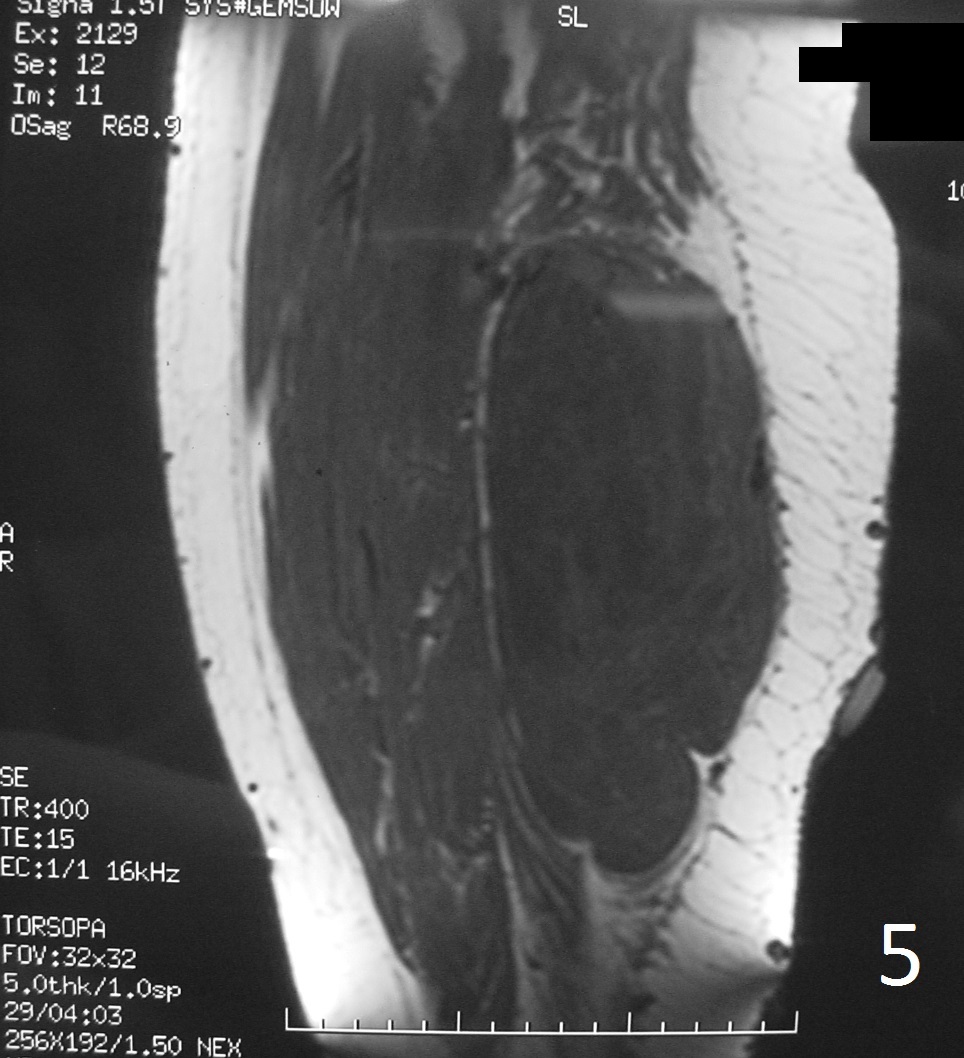
Fig. 5

Fig. 6
Fig 4-6: T2W FS demonstrates same features (Fig. 4) . Sagittal T1W (Fig. 5) and T1W FS (Fig. 6) of same case.

Fig. 7
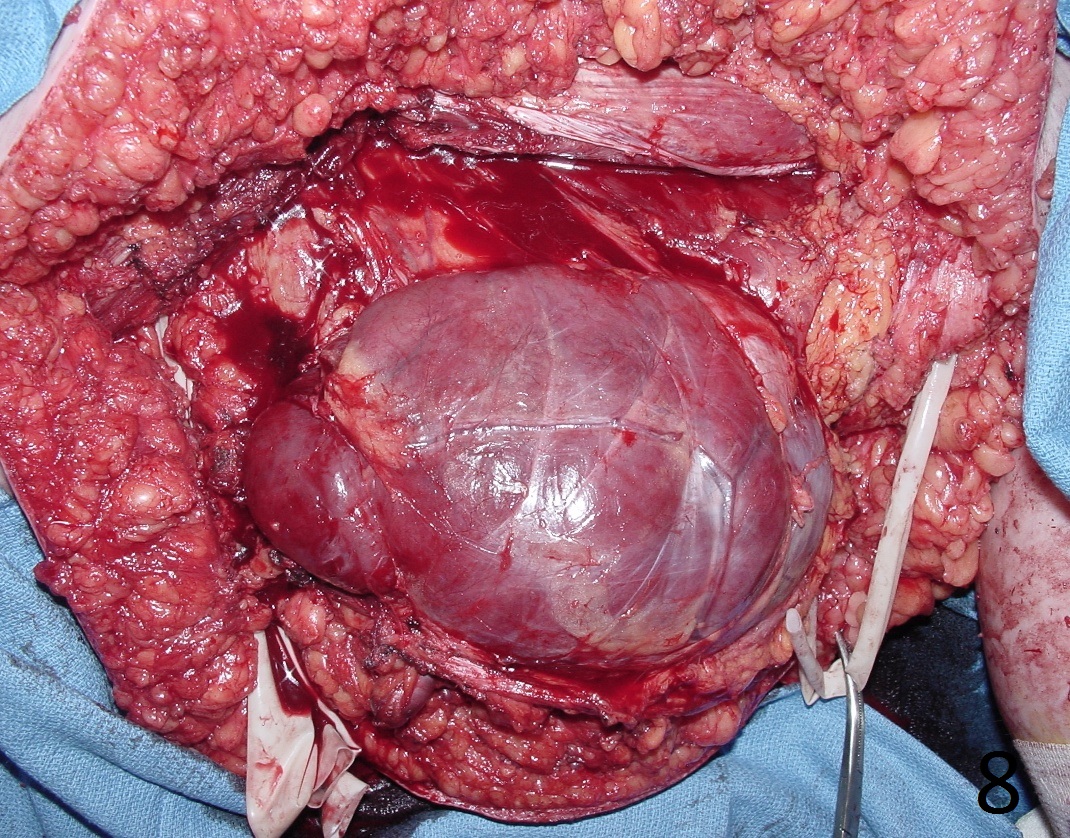
Fig. 8
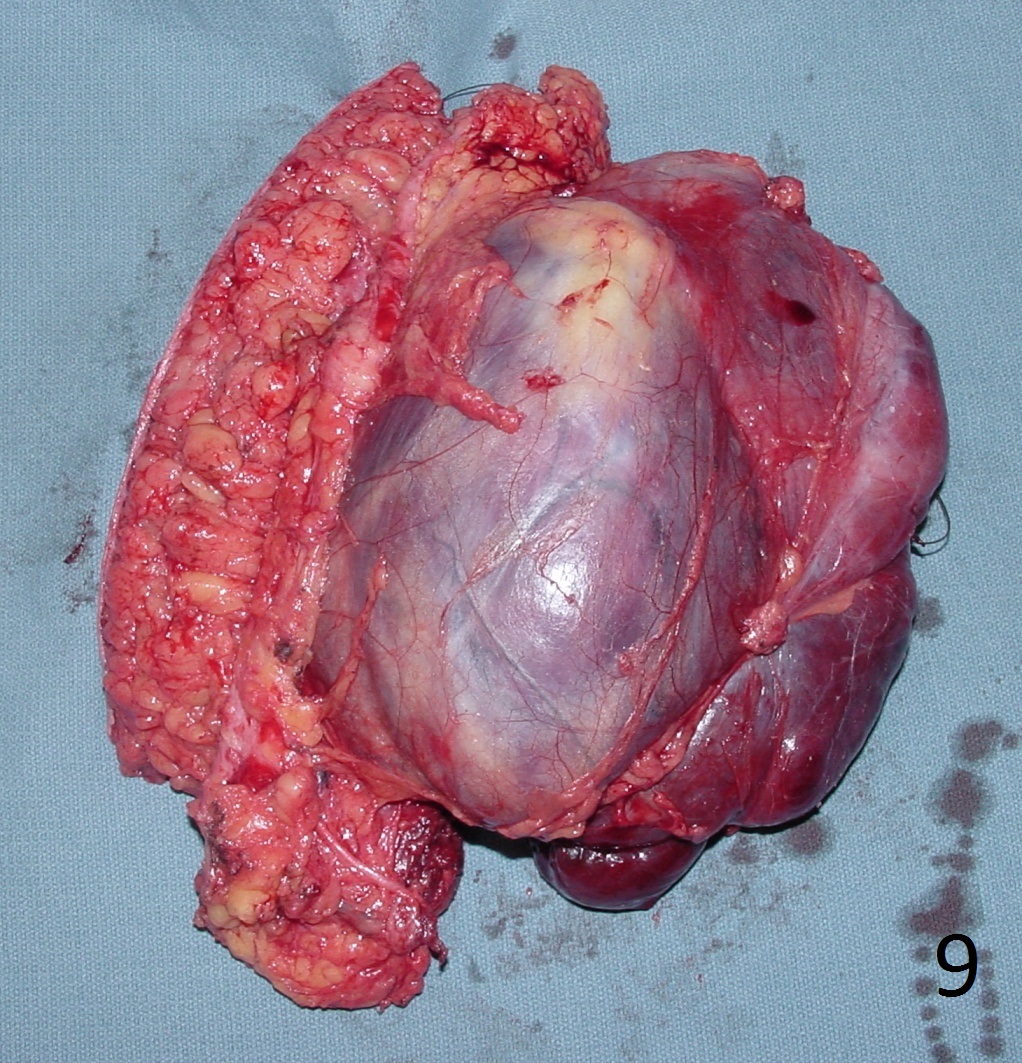
Fig. 9
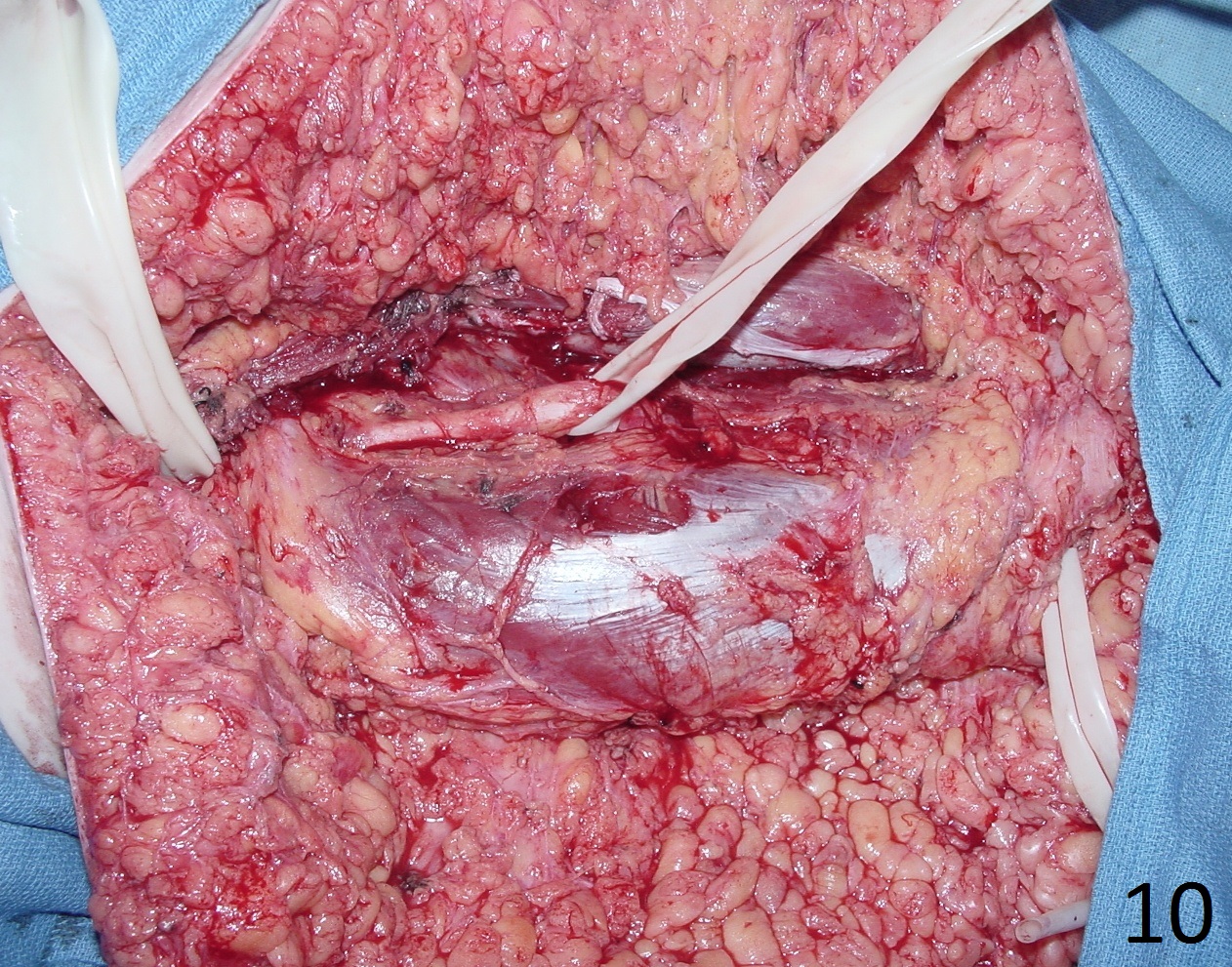
Fig. 10
Fig. 7-10: Intraoperative photographs show radical resection of the solitary fibrous tumor in the thigh area (Fig. 7-10) The tumor was separated from the sciatic nerve and the sciatic nerve was preserved (Fig. 10)
