GENERAL INFORMATION
Liposarcoma is one of the most commonly diagnosed soft tissue sarcomas, accounting for approximately 12.8% of all sarcomas. Most patients are older than 50 years of age who complain of a large, painless, deep-seated mass located proximally in the extremities.
Liposarcoma is a malignant mesenchymal neoplasm composed of lipogenic tissue with varying degrees of atypia. MRI is nonspecific except for well-differentiated tumors in which fat signal is easily distinguished. Different types of Liposarcoma have been described depending on their histology, including; well-differentiated liposarcoma (40%), myxoid liposarcoma/round cell liposarcoma (30%), pleomorphic (15%) and dedifferentiated liposarcoma (5%), each with different clinical behavior.
Myxoid Liposarcoma
Myxoid Liposarcoma (MLPS) is the second most common group of adipocytic/lipogenic sarcomas accounting for about 30% to 35% of all liposarcomas. It is a malignant tumor histologically characterized by round to oval mesenchymal cells, small signet ring lipoblasts, and rich network of capillaries in a myxoid stroma. Both myxoid and round cell liposarcomas have the same genetic translocation. It is believed that these two entities are intimately related and represent a spectrum of the disease with the theory that myxoid liposarcomas can transgress into round cell liposarcoma which is a more aggressive neoplasm with much greater potential for metastasizing. Round cell liposarcomas appear similar to a myxoid liposarcoma except that myxoid stroma is not present.
These tumors nearly always occur in adults but can present in a younger aged population more frequently than the other types of liposarcomas. There is no gender predilection. They arise most commonly in the deep soft tissues of the proximal extremities and the retroperitoneum.
CLINICAL DATA
•
Rare; less than 2 per 1,000,000 people
•
Can occur in younger patients compared to other types of Liposarcoma
•
No gender predilection.
•
Commonly arises in the deep soft tissue of proximal extremities, within the musculature of the thigh.
•
Rare in the retroperitoneum
Differential diagnosis
•
Different types of Liposarcoma
•
MFH
•
Myxoid chondrosarcoma
•
Myxoma
•
Ganglion
•
Synovial cyst/bursa
•
Peripheral nerve sheath tumor
•
Lipoma
•
Other sarcomas (e.g. fibrosarcomas , leiomyosarcoma)
CLINICAL PRESENTATION
Signs/Symptoms
Rapidly enlarging, painless mass. 30% of patients may have dull aching pain or tenderness.
Some patients report trauma in the affected area (trauma does not cause MFH) and the MFH may be misconstrued as a hematoma or muscle strain
Systemic symptoms are not expected.
Prevalence
Male predilection (70%)
More frequent in caucasion population
Age
Most cases occur between 50 and 70 years old.
Extremely rear in children.
Sites
Lower extremity
50%
Most commonly arises in the thigh
Upper Extremity
25%
Retroperitoneum
15%
Head/neck
5%
RADIOGRAPHIC PRESENTATION
•
Variable sizes, may reach sizes more than 15 cms.
•
Non homogeneous on MRI or CT
CT
•
Inhomogeneous masses of low density on CT with enhancing areas (Fig. 1)
Patterns based on amount and distribution of fat:
1.
solid - attenuation > + 20 HU
2.
mixed - areas of < -20 HU and areas of > + 20 HU
3.
pseudocystic - homogenous density between – 20 and + 20 HU
CT findings favoring a liposarcoma from a lipoma include
•
Poor definition of adjacent structures
MRI (Fig. 2 and 3)
•
Large well defined multilobulated mass.
•
Low signal on T1 weighted images. Usually adipose tissue composes less than 10 percent of the tumor and is difficult to detect on an MRI as high signal on T1W images. (Fig. 2A)
•
Marked high signal on T2 weighted sequence. (may mimic a synovial cyst) (Fig. 2B) The myxoid/mucinous tissue consists of mucopolysaccharides that holds onto water and shows up high signal on T2W images.
•
Identification of the subtle fat requires comparison of T1W and T2W images in the same plane but is usually very difficult to discern. (Fig. 2)
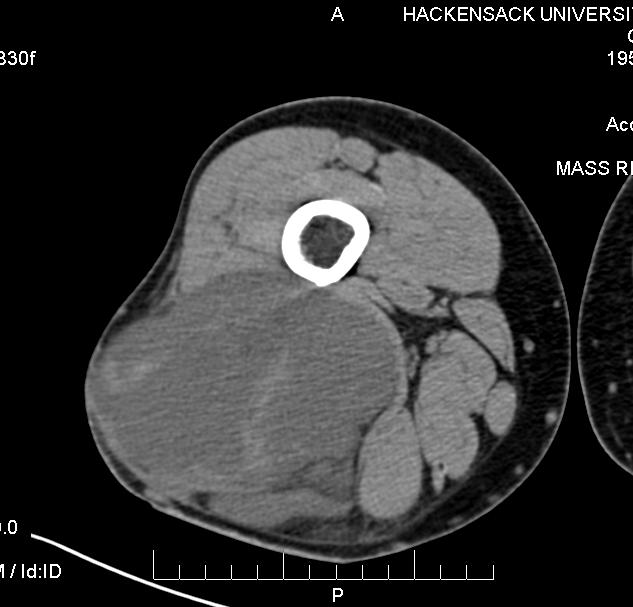
Fig. 1 CT scan image of a myxoid liposarcoma shows an inhomogeneous mass of low density that is located in the posterior compartment of the thigh.
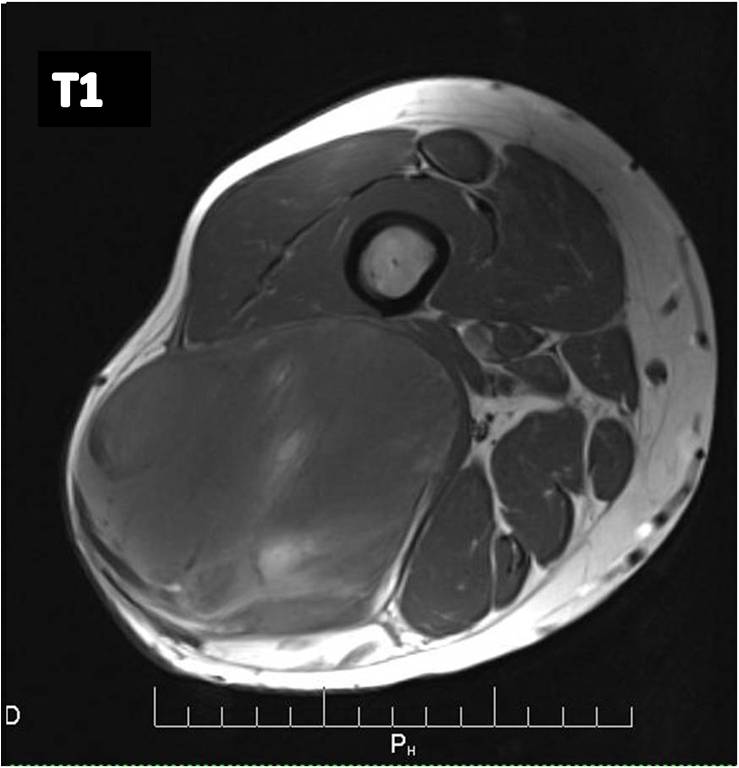
Fig. 2A
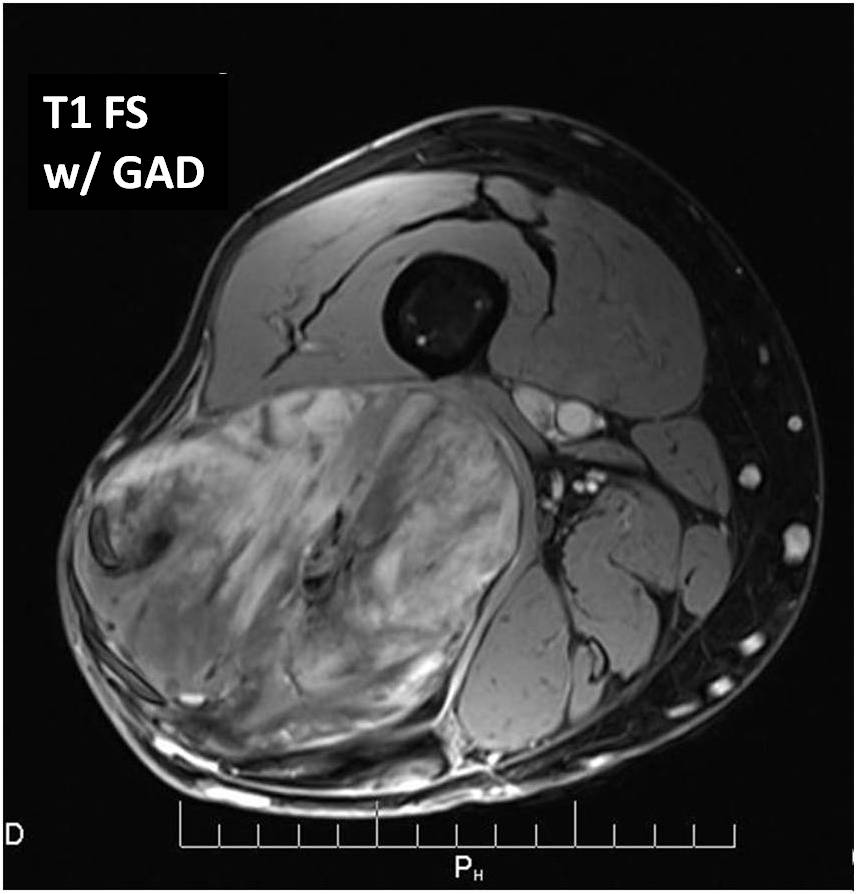
Fig. 2B
Fig 2. T1-weighted MR image (A) of a myxoid liposarcoma demonstrates well-defined mass of intermediate signal intensity with central areas of high intensity. T2 –weighted fat-suppressed image (B) heterogeneously mostly high signal intensity within the lesion.
Fig. 3 T1-weighted post contrast fat-suppressed images show heterogeneous increased signal and enhancement within the tumor. The fatty component is less than 10%
PATHOLOGY
Gross Pathology (Fig. 4)
•
Multinodular tumor
•
Gelatinous cut surface in low grade tumors.
•
White yellow areas represent the Round Cell (RC) component (high grade areas)
 Fig. 4 Gross Pathology Myxoid Liposarcoma. Multinodular intramuscular tumor. Fleshy areas represent the Round Cell (RC) component (high grade sarcoma). The surface is usually glistening from the myxoid component.
Microscopic Pathology
Fig. 4 Gross Pathology Myxoid Liposarcoma. Multinodular intramuscular tumor. Fleshy areas represent the Round Cell (RC) component (high grade sarcoma). The surface is usually glistening from the myxoid component.
Microscopic Pathology (Fig. 5 and Fig. 6)
•
Univacuolar and multivacuolar lipoblasts admixed with round appearing cells in myxoid ground substance.
•
Acute angular branching capillary vasculature
•
FUS-CHOP Fusion gene, PI3K mutation (<20%)
•
77% of myxoid liposarcomas are associated with a chromosomal translocation t(12;16) q(13;p11)
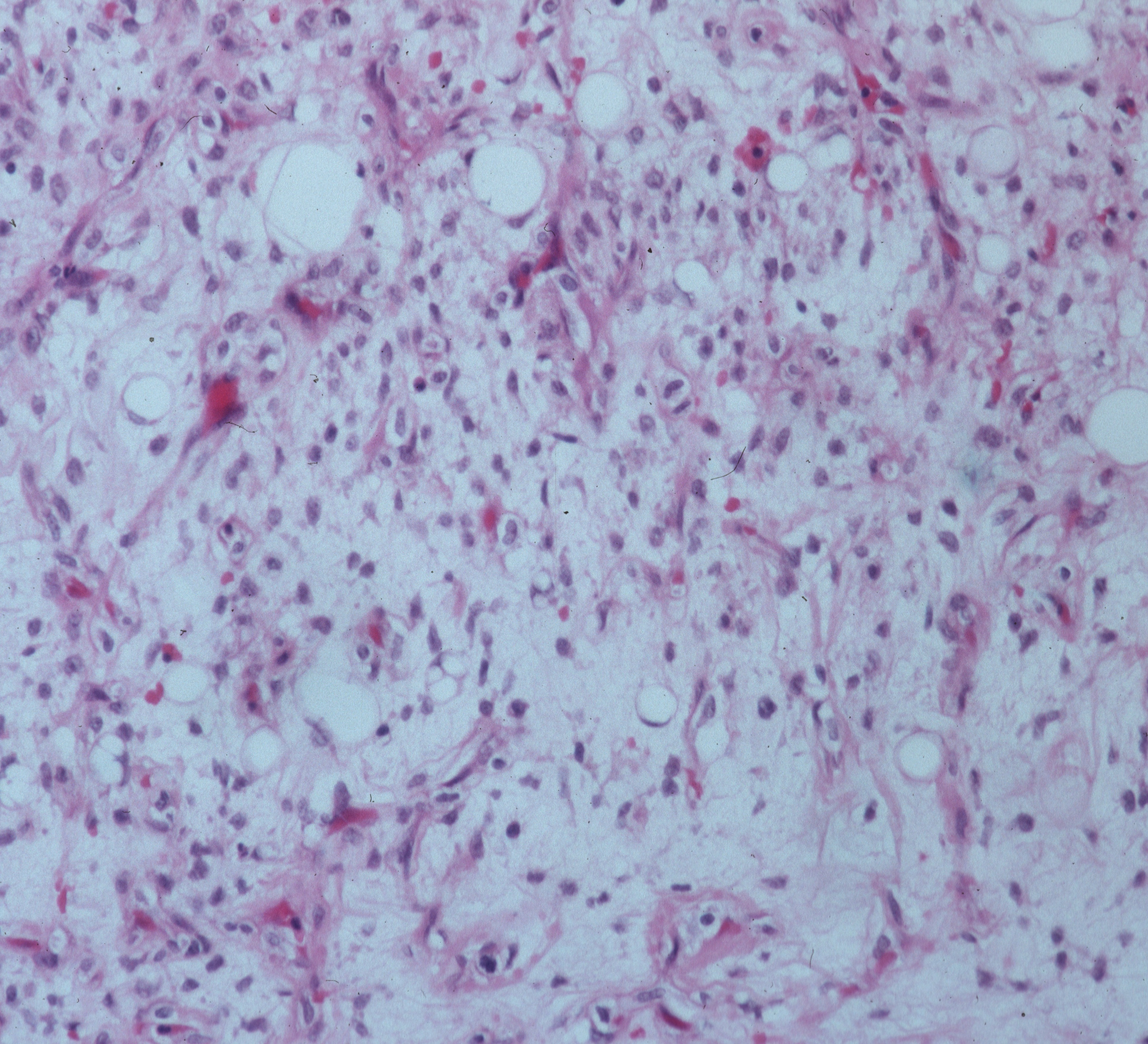
Fig. 5
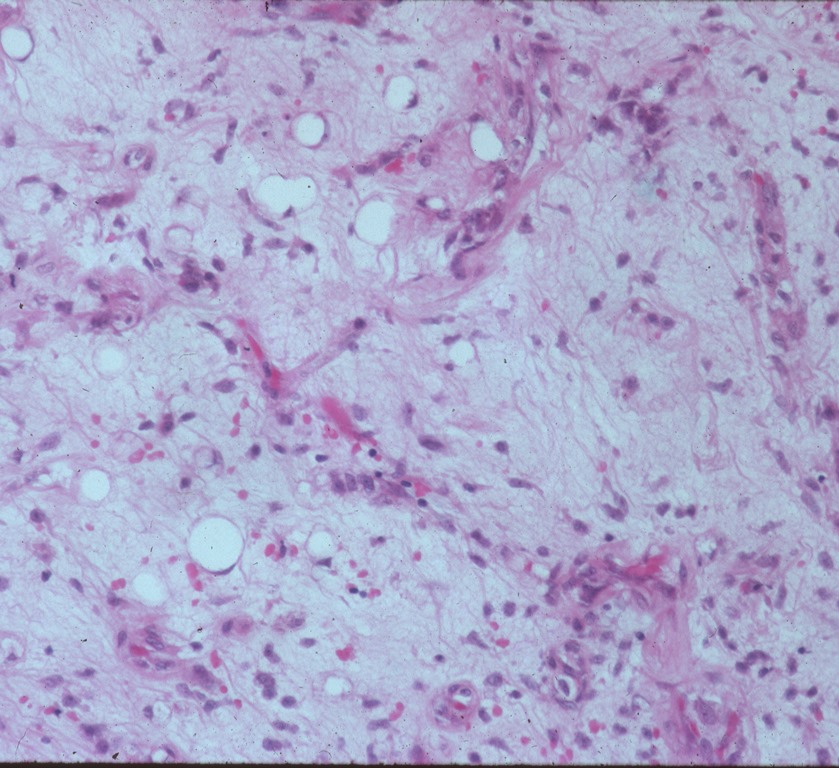
Fig. 6
Fig. 5 and 6 Microscopic Pathology. Low (5) and High (6) magnification H&E slides. Darkly stained but uniform oval cells immersed in a myxoid and lipomatous stroma. Capillary vasculature is abundantly present.
PROGNOSIS
Biological Behavior
•
MLPS have shown 69 – 100% of disease-specific survival
•
High risk of local recurrence (7-28%)
•
1 in 3 patients present with metastases and often occurs in unusual sites before metastasizing to the lungs, such as;
o
Soft tissue (retroperitoneum, opposite extremity, axila, etc)
o
Bone (spine)
•
Important prognostic factors are age of the patient and presence of Round cell component
•
The presence of hypercellularity or round cell differentiation is associated with worsening of prognosis and higher rate of metastases.
•
The prognosis for multifocal myxoid liposarcoma is always poor.
TREATMENT
•
Standard treatment is wide surgical resection. (Fig. 7, 8, 9 and 10)
•
In selected patients, adjuvant therapy (radiotherapy, chemotherapy, or both) may be indicated.
•
Amputation for unresectable tumors
 Fig. 7
Fig. 7
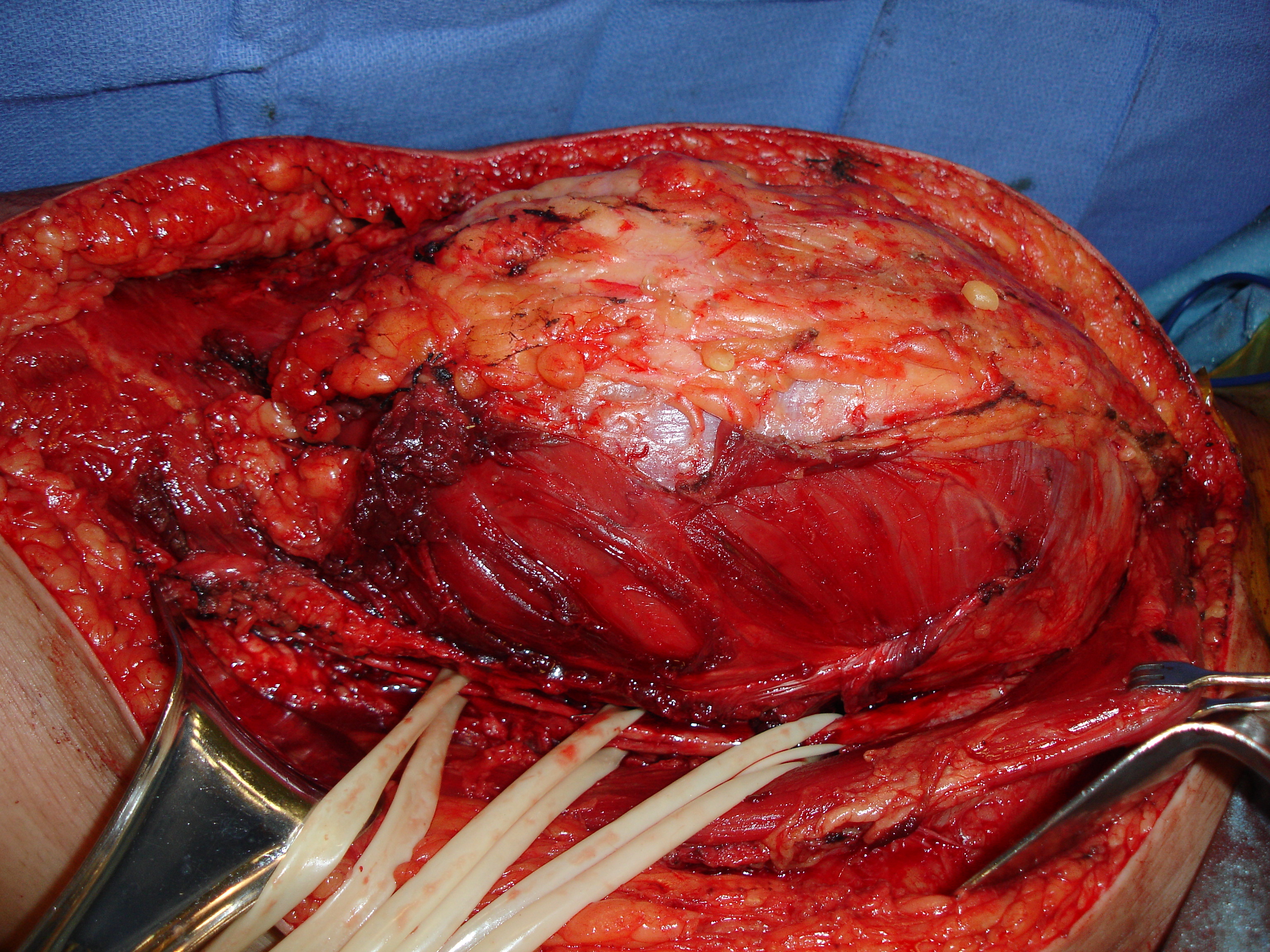 Fig. 8
Fig. 8
Fig. 9
Fig. 7, Fig. 8 and Fig. 9 Intraoperative photos show a radical resection of a myxoid liposarcoma from the thigh.
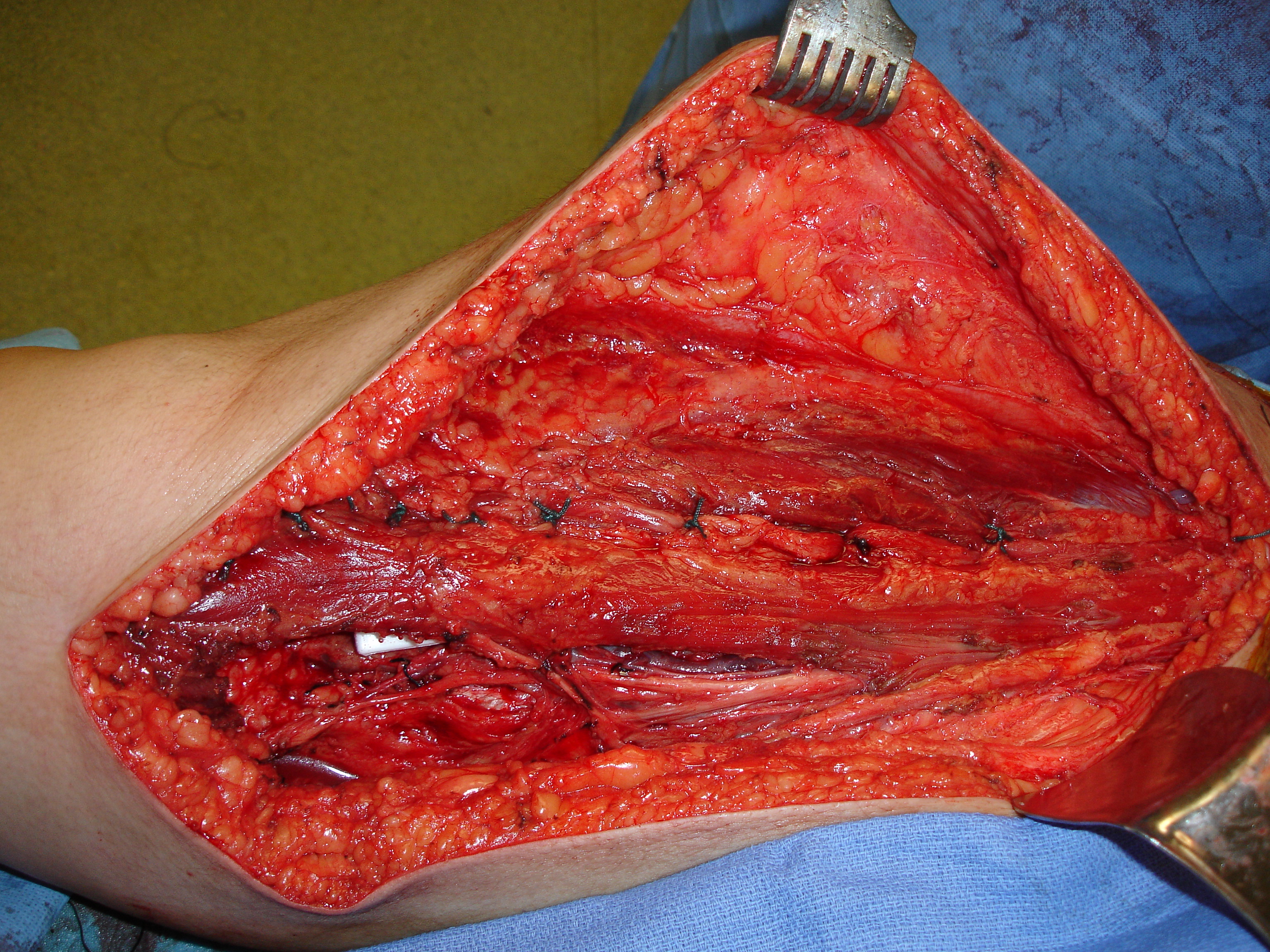
Fig. 10 Intraoperative photo shows muscle flap rotation for closure of the dead space after tumor removal.
