GENERAL INFORMATION
Benign tumor composed of mature adipocytes with uniform nuclei identical to the cells of normal adult fat. Lipoma is the most common tumor of soft tissue.
Benign/Mature adipocytes have cytoplasmic lipid in a single large vacuole that pushes the nucleus to the periphery of the cell and compresses it into a thin crescent.
Lipoblasts: Malignant or Immature adipocytes. Have larger peripheral or central nucleus indented by one or more fat vacuoles so that spikes of chromatin project between fatty vacuoles. Usually smaller and have smaller vacuoles than mature lymphocytes
CLINICAL DATA
• Most common soft-tissue tumor
•
Common between 40 and 60 years of age
•
Their presentation is more frequent in obese individuals
•
Lipomas are extremely rare in children
•
Most common sarcoma after radiation.
•
Homogeneous tumor in histology and prognosis
•
5% of patients have multiple lipomas
•
Very low rate of recurrence
Differential diagnosis
• Lipoma vs atypical lipomatous tumor (well differentiated liposarcoma)
• Both may look very similar on MRI
• Well differentiated liposarcoma:
• Larger nuclei
• Lipoblasts
• Considerable variation in fat cell size
CLINICAL PRESENTATION
Signs/Symptoms
• Usually appear as slow growing, soft, asymptomatic mass
• Larger lipomas can give symptoms related to the compression of peripheral nerves.
• Some patients may have multiple lipomas.
• Lipomas are more common in obese individuals
• Other factors which can lead to lipoma:
• Diabetes
• Elevated serum cholesterol level
• Blunt, bruising injuries
• Radiation
Prevalence
• Do not display any clear race or sex predilection
Age
• More common in adults over the age of 45, as fat begins to accumulate.
• Extremely rare in children.
Sites
• Subcutaneous lipomas are the most frequent.
• Subcutaneous lipomas are usually found on the back, neck, shoulder, abdomen, or proximal extremities
• Subcutaneous lipomas are uncommon on the hands, feet, or distal extremities
• Nonsubcutaneous lipomas are less common and can be found in many tissues throughout the body
• Intramuscular lipomas are usually found on trunk, large muscles of arm, thigh, shoulder. They must be differentiated from low grade liposarcomas (well differentiated liposarcomas)
• Fatty masses in the retroperitoneum are not lipomas.
RADIOGRAPHIC PRESENTATION
• Subcutaneous Homogeneous Mass
• Average size of 5 to 10 cm
• Regions of mineralization may be demonstrated rarely in plain x-rays particularly if the mass has been injured and has undergone necrosis
• A thin capsule and very thin septations (< 2 mm) are often seen
Plain X-ray
• Radiolucent soft tissue mass
• Calcification may be present particularly in areas of fatty necrosis
CT scan
• Well defined, homogeneous
• No enhancement following contrast administration
• Tissue Attenuation Coefficient is Low (-65 to -120 HU)
• May delineate a fibrous capsule in well encapsulated tumors (attenuation similar to muscle)
MRI
• Follows the signal characteristics of subcutaneous fat on all sequences
• T1: High Signal
• T2: Intermediate Signal; Low Signal with Fat Suppression
• Minimal or No enhancement with gadolinium
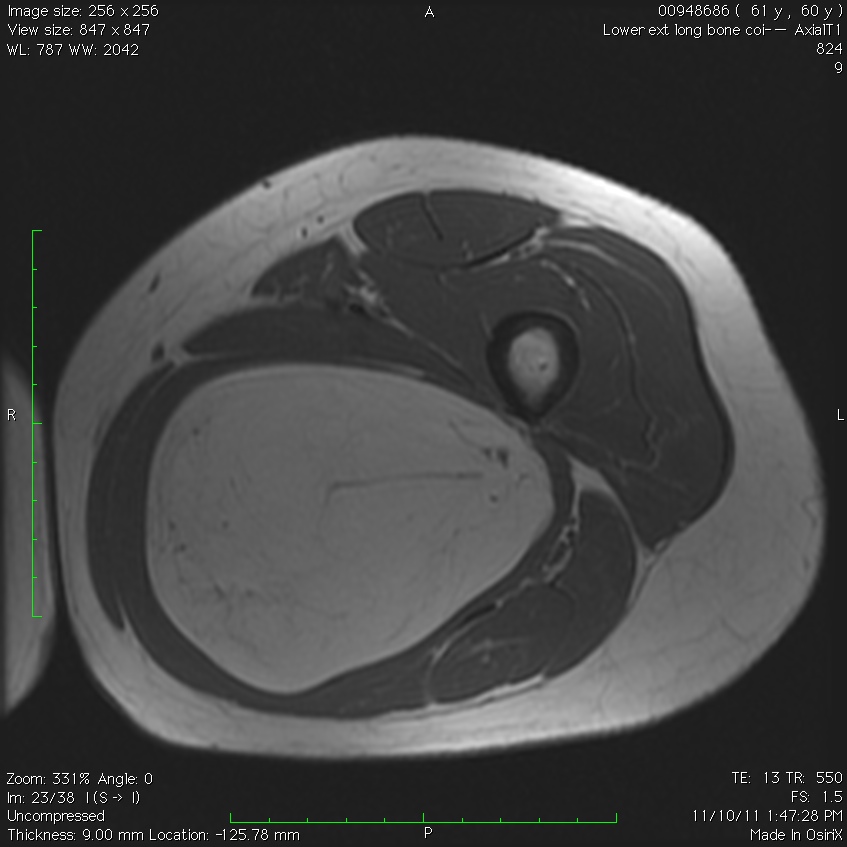 Fig. 1A
Fig. 1A
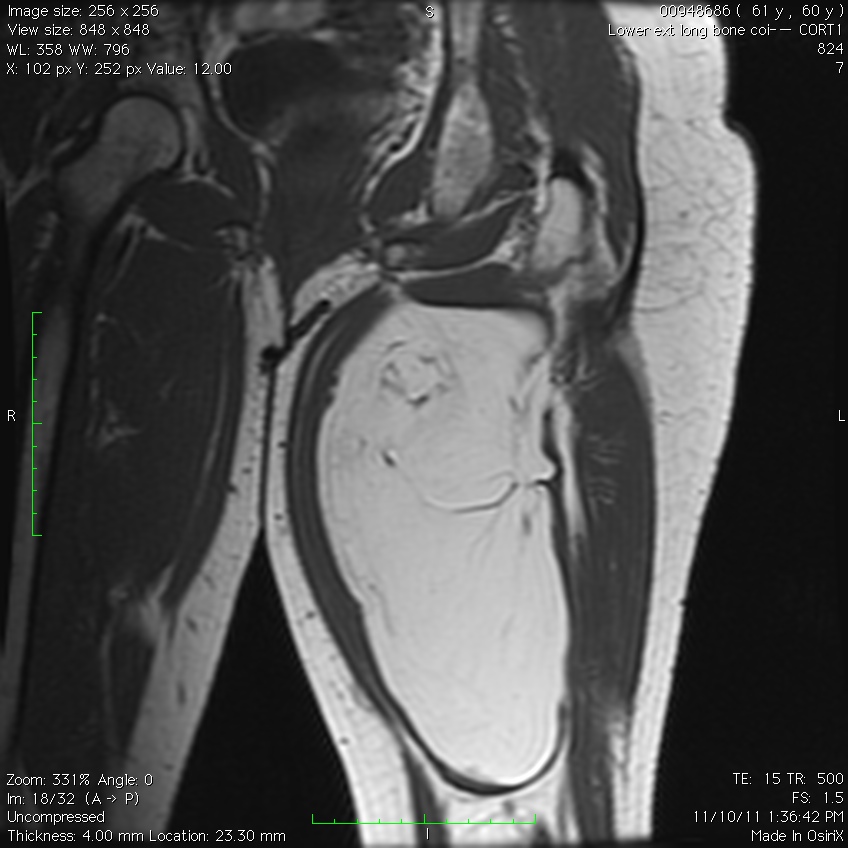 Fig. 1B
Fig. 1B
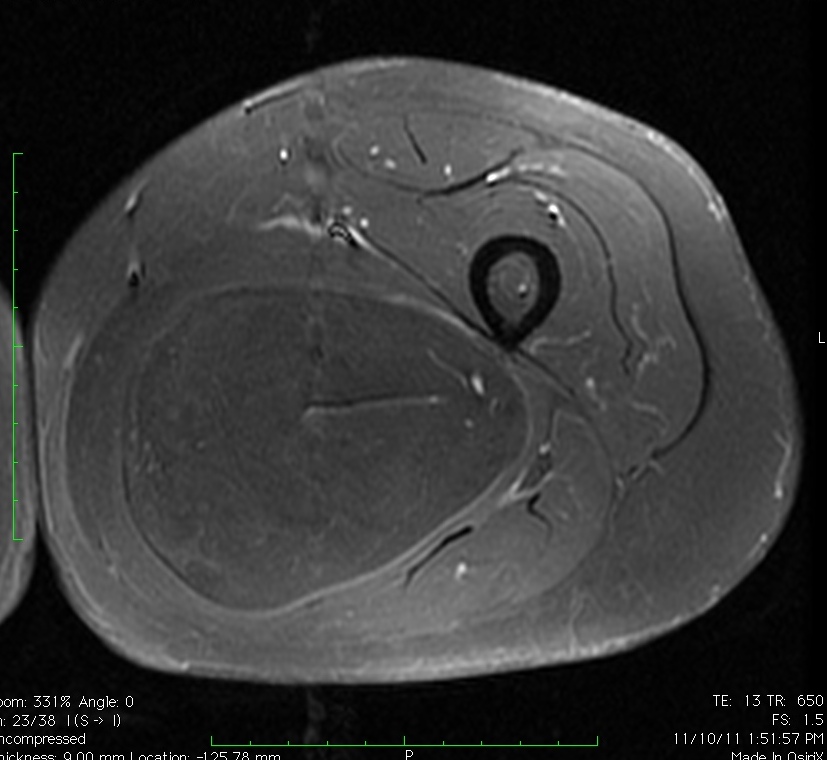
Fig. 1C
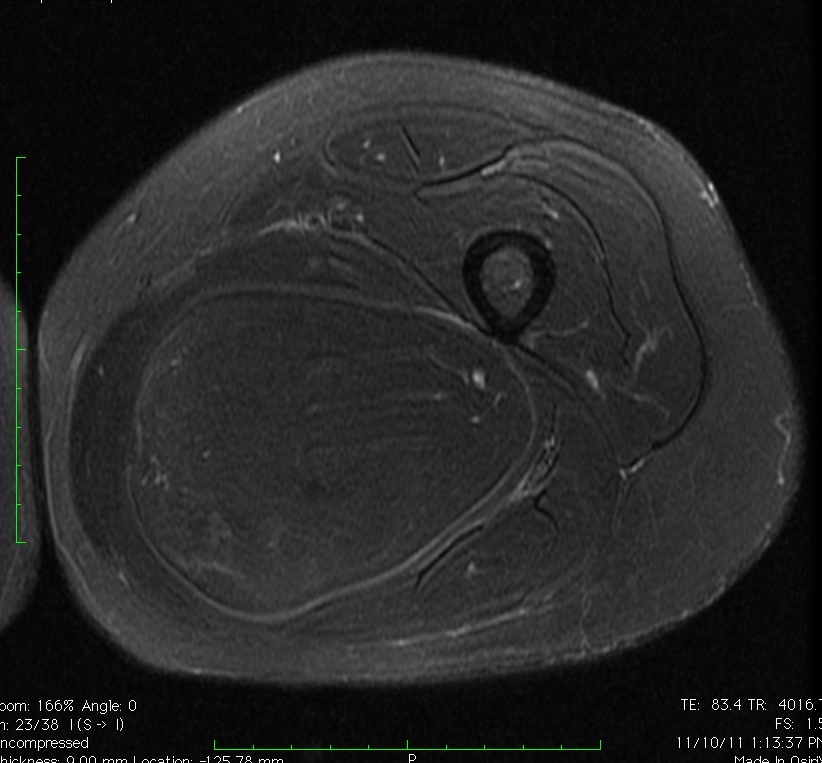
Fig. 2A
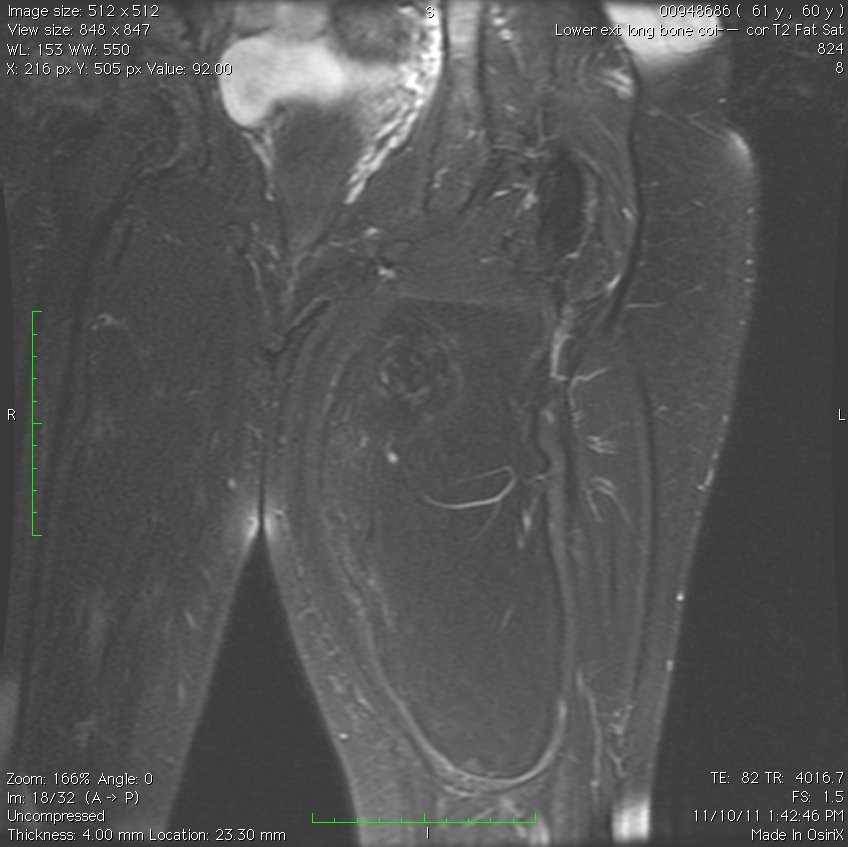
Fig. 2B
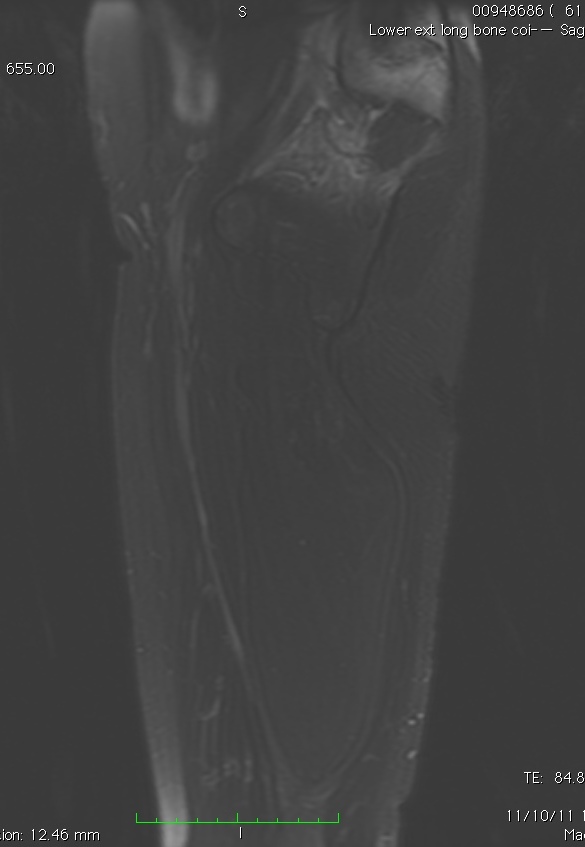
Fig. 2C
Fig. 1A, 1B, 1C, 2A, 2B, 2C: MRI of a lipoma: T1- weighted images shows an homogeneous mass in the posterior compartment of the thigh with high signal, saturates on fat saturated sequences with no or minimal enhancement. On T2-weighted images demonstrate an intermediate signal on FSE T2, saturates (becomes dark) on fat saturated sequences.
PATHOLOGY
Gross
• Soft yellow fatty mass indistinguishable from normal fat
• Well circumscribed
• Lobular growth in some lipomas
• May have a significant fibrous component reflected as white tissue
• Muscle fibers may be present with intramuscular lipomas
Microscopic
• Mature fat cells with small, uniform, eccentric nuclei
• Nucleus compressed against the periphery of the cell membrane by a fat vacuole
• No mitotic figures
• Can have areas that undergo fat necrosis
• Muscle fibers interspersed amongst mature adipocytes (intramuscular lipomas)
• Other components
• Fibrous tissue
• Myxoid tissue
• Blood vessels
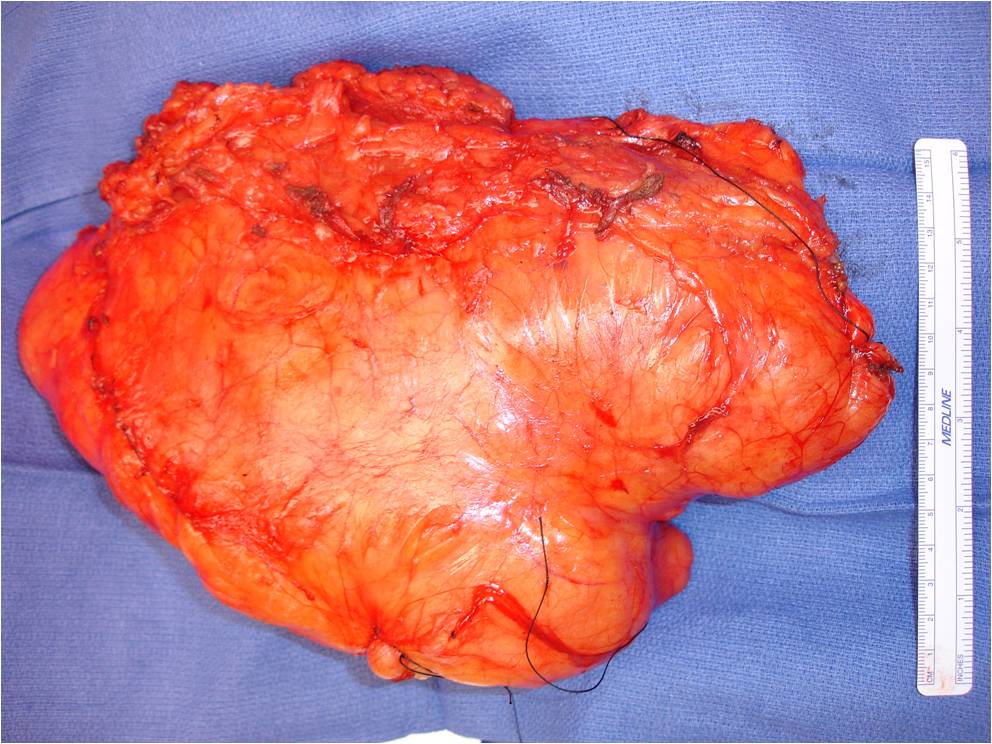 Fig. 3: Gross pathology of a lipoma demonstrates a big well circumscribed yellow fatty mass indistinguishable from normal fat with lobular growth.
Fig. 3: Gross pathology of a lipoma demonstrates a big well circumscribed yellow fatty mass indistinguishable from normal fat with lobular growth.
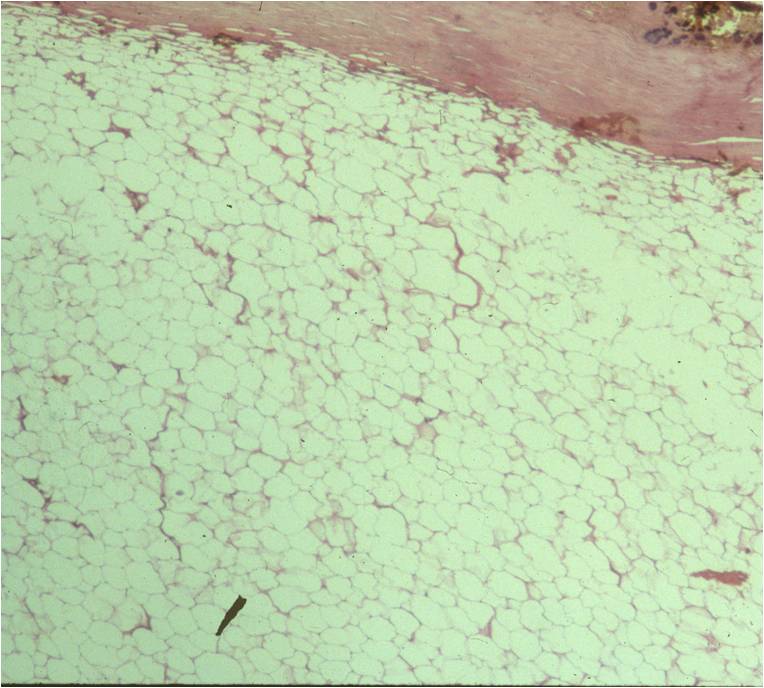 Fig. 4
Fig. 4
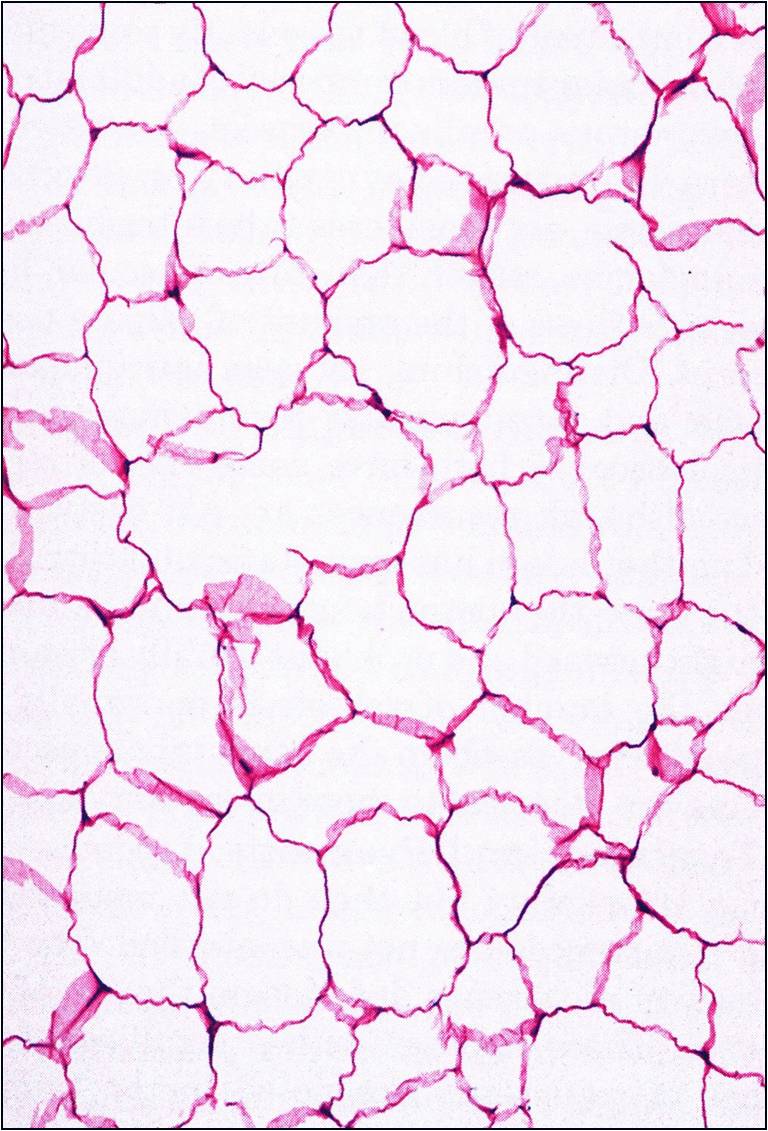
Fig. 5
Fig. 4 & 5: Microscopic Pathology of a lipoma shows a homogeneous structure in low and high magnification with a uniform cell pattern and peripheral compressed nuclei barely discernible. Mature adipocytes. No mitoses.
PROGNOSIS
Biological Behavior
• Lipomas are benign
• Malignant changes are extremely rare
• Recurrence rate is less than 5% after local excision
• No metastases
TREATMENT
• Marginal excision for symptomatic, large or deep lesions is the mainstay therapy for lipomas.
• Observation for small asymptomatic lipomas
• Lipomas are benign and do not metastasize and therefore are not treated with any forms of chemotherapy nor radiation.
• Local recurrence risk depends on size and location of lipoma
• Local recurrence rarely occurs for subcutaneous tumors
• Intramuscular tumors associated with up to 20% local recurrence rate.
 Fig. 6A
Fig. 6A
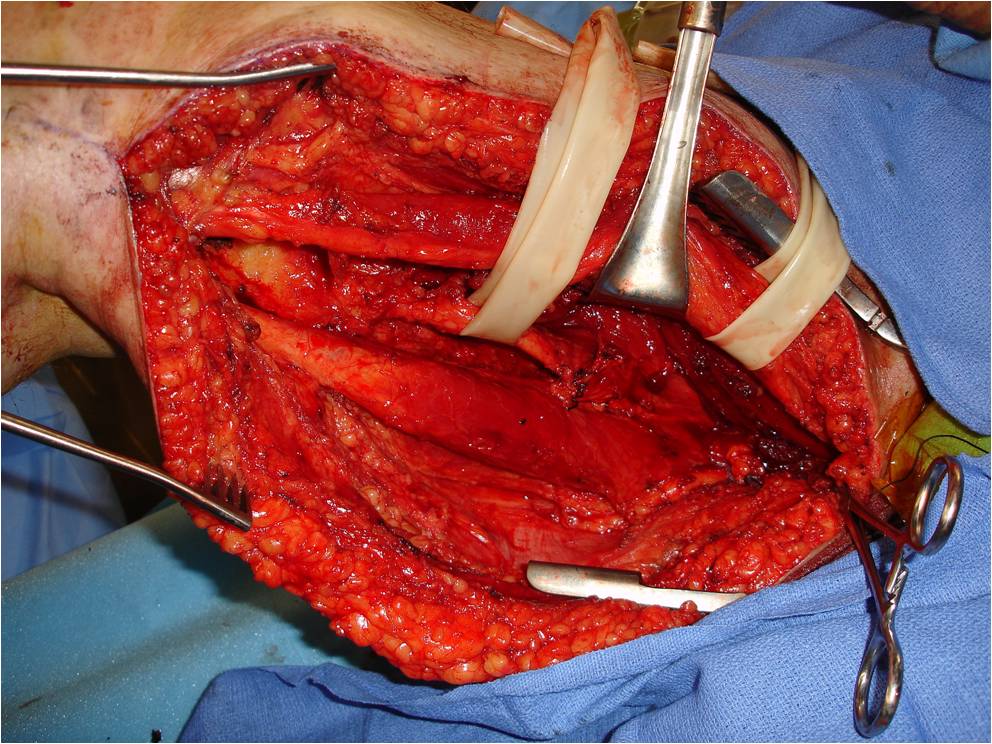
Fig. 6B
