Dedifferentiated Liposarcoma
GENERAL INFORMATION
Liposarcoma is one of the most commonly diagnosed soft tissue sarcomas, accounting for approximately 12.8% of all sarcomas. Most patients are older than 50 years of age and most patients complain of a large, painless, deep-seated mass usually located proximally in the extremities. Liposarcoma is a malignant mesenchymal neoplasm composed of lipogenic tissue with varying degrees of atypia. MRI is nonspecific for evaluating liposarcomas except for well-differentiated tumors in which fat
signal is easily distinguish. Different types of Liposarcoma have been described depending of their histology, including; well-differentiated liposarcoma (40%), myxoid liposarcoma/round cell liposarcoma (30%), pleomorphic (15%) and dedifferentiated liposarcoma (5%) each with different clinical behavior. Well-differentiated liposarcoma is commonly referred to as an atypical lipoma or low grade liposarcoma.
Dedifferentiated Liposarcoma (DDLPS)
Dedifferentiated liposarcoma is the least common subtype of liposarcoma and usually arises from a well-differentiated liposarcoma (WDLPS). Progression occurs
in 17 % of patients when WDLPS is located in the retroperitoneum and 6% of cases when WDLPS is located in the extremities. Dedifferentiated liposarcoma has also been defined as an atypical liposarcoma that progresses or changes over course of time with variable histologic grade. This is essentially a low grade liposarcoma admixed with a high grade spindle cell sarcoma. These tumors occur mostly in adults and tend to grow more aggressively than a low grade well differentiated liposarcoma. They arise most commonly in the retroperitoneum.
CLINICAL DATA
•
18 % of Liposarcomas
•
Most commonly occurs in patients over 50 years old
•
No gender predilection
•
Commonly on deep soft tissue of retroperitoneum and proximal extremities
•
Progresses from WDLPS and their presentation is more frequent after a recurrence of WDLPS.
•
Up to 17% of well differentiated LPS progresses to DDLPS
DIFFERENTIAL DIAGNOSIS
Different types of Liposarcoma
•
MFH
•
Synovial Sarcoma
•
Lipoma
•
Other sarcomas (e.g. fibrosarcomas, other sarcomas (e.g. fibrosarcoma, leiomyosarcoma)
•
Fat containing masses in the retroperitoneum (e.g. angiomyolipoma, myelolipoma)
CLINICAL PRESENTATION
Signs/symptoms
•
Painless enlarging mass
•
Can attain a very large size
•
More locally aggressive than WDLPS.
•
Metastasis rate, range from 13% to 47%
Prevalence
•
No gender prevalence
Age
•
Most cases are diagnosed in the 6th decade of life
•
Rare in children.
Sites
•
Retroperitoneum
•
Lower extremities
•
Upper extremity
•
Trunk
RADIOGRAPHIC PRESENTATION
Slow growth
•
Variable sizes, normally more than 10 cms.
•
Thick internal septations
•
Focal nodules of sarcomatous degeneration larger than 1cm on MRI
MRI
•
Large encapsulated lipomatous mass with
multiple thick internal trabeculations. (Fig. 1 – 13)
•
High signal intensity both on T1-weighted and T2 weighted (Fig. 3)
•
Signal loss on FS T1 weighted images, and focal nodules(>1 cm is suggestive of a DDLS). (Fig. 1 & 7)
•
Low intensity images are visible in case of Hemorrhage.
•
Contrasted images show hyper-enhancement of the tumors. (Fig. 4, 5, 11-13)
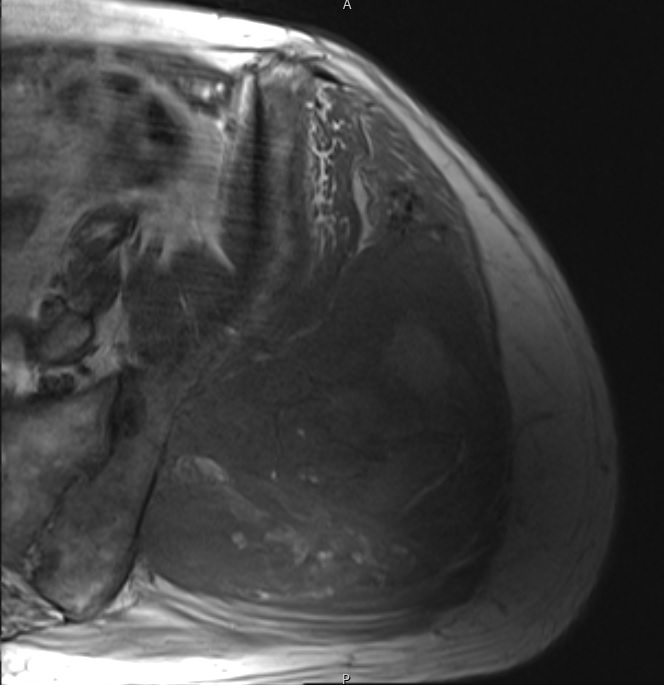 Fig. 1
Fig. 1
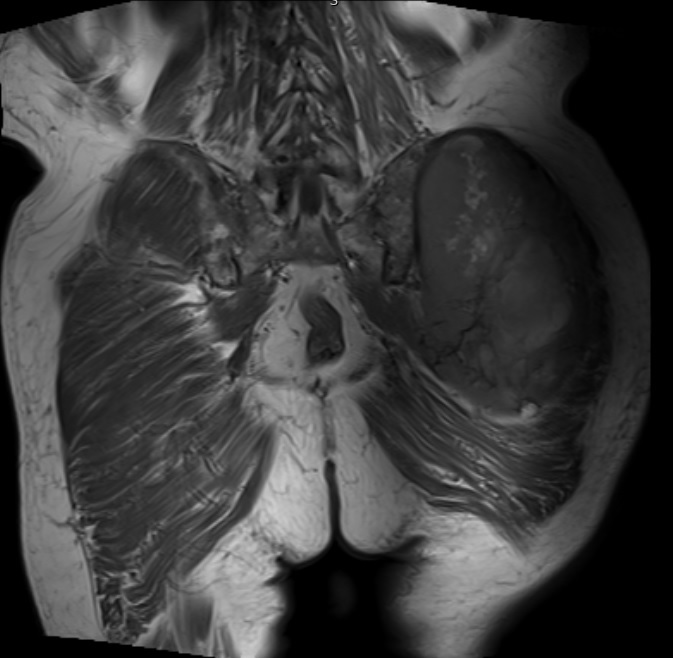 Fig. 2
Fig. 2
Fig. 1 & 2 Magnetic Resonance Image shows a large heterogeneous mass in the left gluteal region with low intensity signal on Axial (Fig. 1) and Coronal (Fig. 2) T1-weighted images admixed with some high signal areas indicative of fatty tissue. Higher intensity signal is visible compatible with hemorrhage or necrotic tissue. The mass involve the central portion of the left iliac bone.
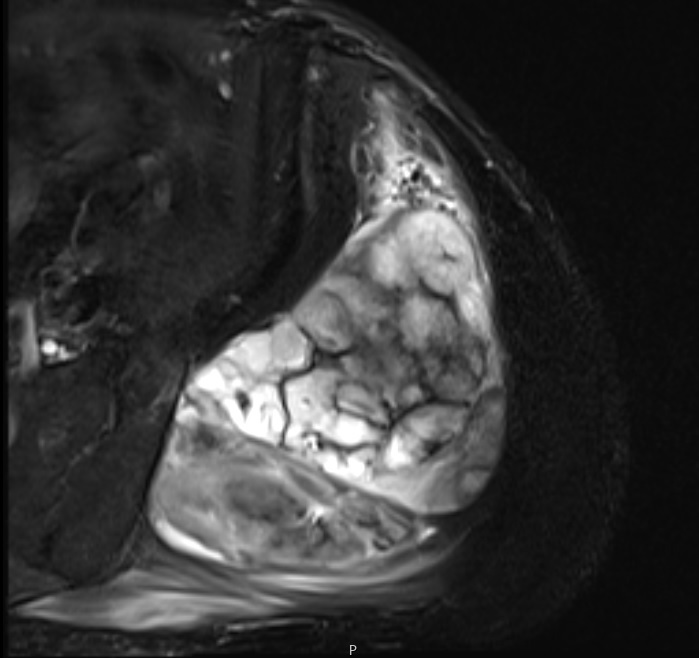 Fig. 3 Axial fat suppressed T2-weighted MR image demonstrates a large heterogeneous mass with multiple thick internal trabeculations. Fatty areas suppress on T2 weighted fat suppressed areas
Fig. 3 Axial fat suppressed T2-weighted MR image demonstrates a large heterogeneous mass with multiple thick internal trabeculations. Fatty areas suppress on T2 weighted fat suppressed areas
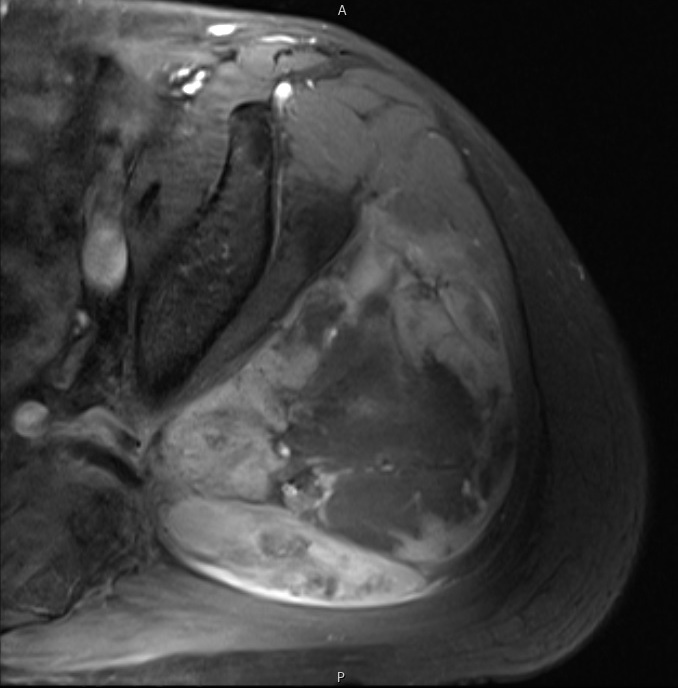
Fig. 4
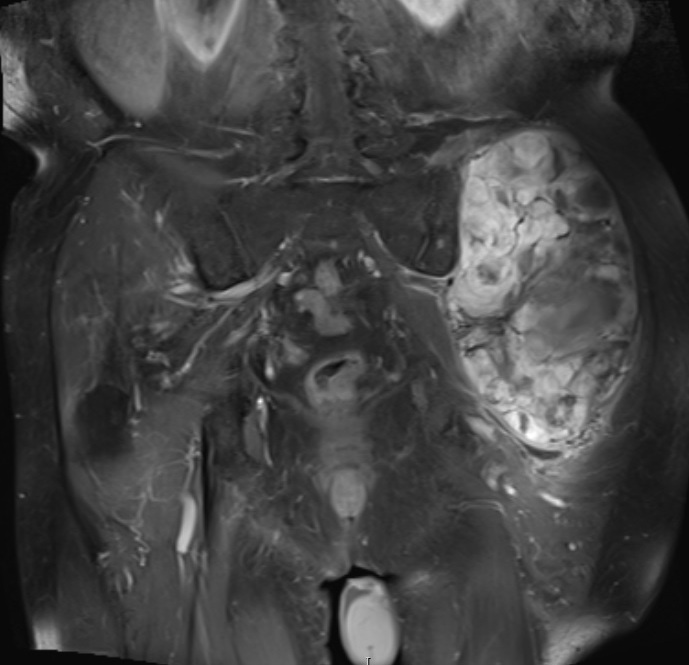
Fig. 5
Axial (Fig. 4) and Coronal (Fig. 5) contrasted T1-weighted MR images show a large heterogeneous mass with central and peripheral enhancement. Central low signal intensity image is compatible with necrosis and hemorrhage.
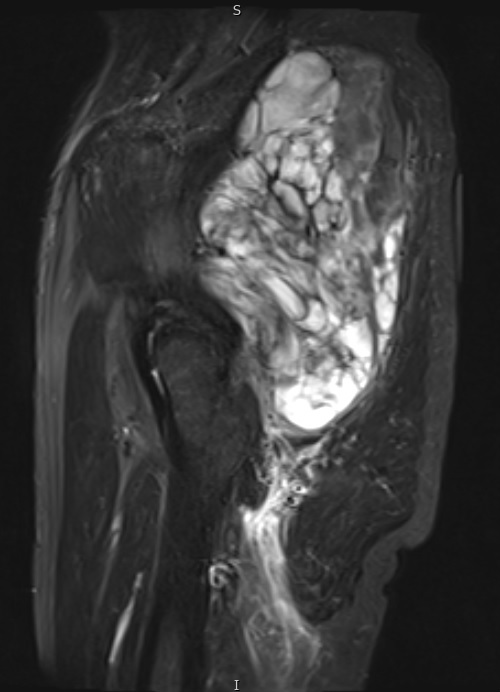
Fig. 6 Fig. 6 STIR MR image demonstrates a large mass in the gluteal region with some enhancing tissue posterior to the trochanteric area which may reflect reactive edema.

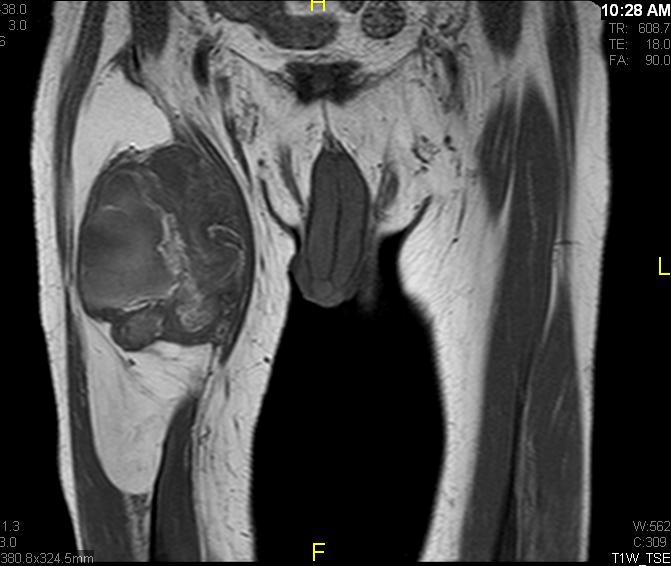
Fig. 7 & 8 Magnetic Resonance Image shows a large heterogeneous mass in the right thigh with low intensity signal on Axial (Fig. 7) and Coronal (Fig. 8) T1-weighted images admixed with high signal areas. The high signal areas represent low grade fatty tissue and low signal the dedifferentiated areas. Higher intensity signal is visible compatible with hemorrhage or necrotic tissue.

Fig. 9 Coronal fat suppressed T1-weigthed MR image demonstrates a large heterogeneous mass in the anterior compartment of the thigh with some areas suppressed corresponding with fatty areas within the tumor. Central hyper enhanced areas compatible with hemorrhage or necrosis.
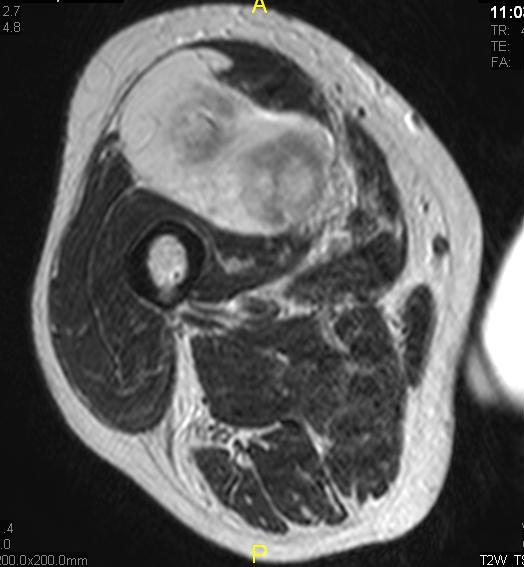
Fig. 10 Axial T2 weighted MR image demonstrates a large well encapsulated heterogeneous mass with multiple thick internal trabeculations located in the anterior compartment of the thigh.
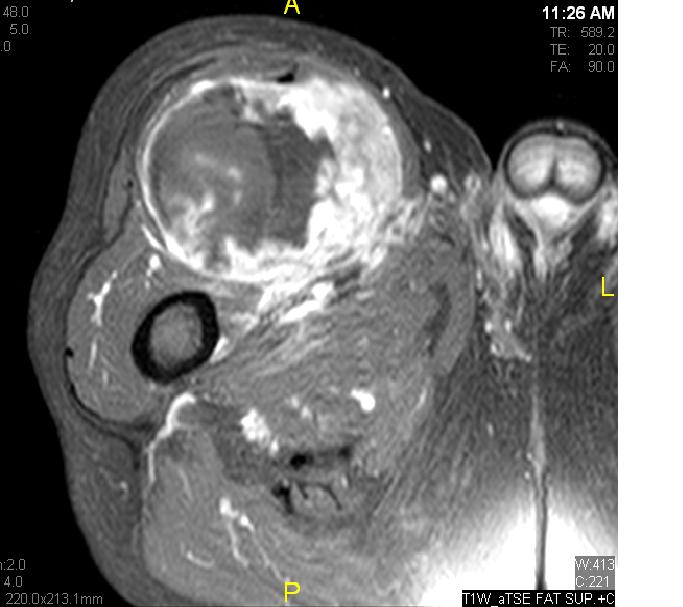
Fig. 11

Fig. 12

Fig. 13
Fig. 11 - 13 Axial (Fig. 11), Coronal (Fig. 12) and Sagital (Fig. 13) contrasted T1-weighted MR images show a large heterogeneous mass with central and peripheral
enhancement. Multiple thick trabeculations. Central low signal intensity image is compatible with necrosis and hemorrhage.
PATHOLOGY
Gross Pathology (Fig. 14)
•
Large yellow masses (WDLPS area)
•
Solid gray (sometimes fleshy) non lipomatous (DDLPS) areas.
Microscopic Pathology
•
Well differentiated liposarcoma (Fig. 15) with a sudden transition to a non-lipogenic sarcoma at least in several millimeters (Fig. 16)
•
Heterogeneous elements in 10%
•
DDLPS as WDLPS overexpresses MDM2 and CDK4 oncogens.
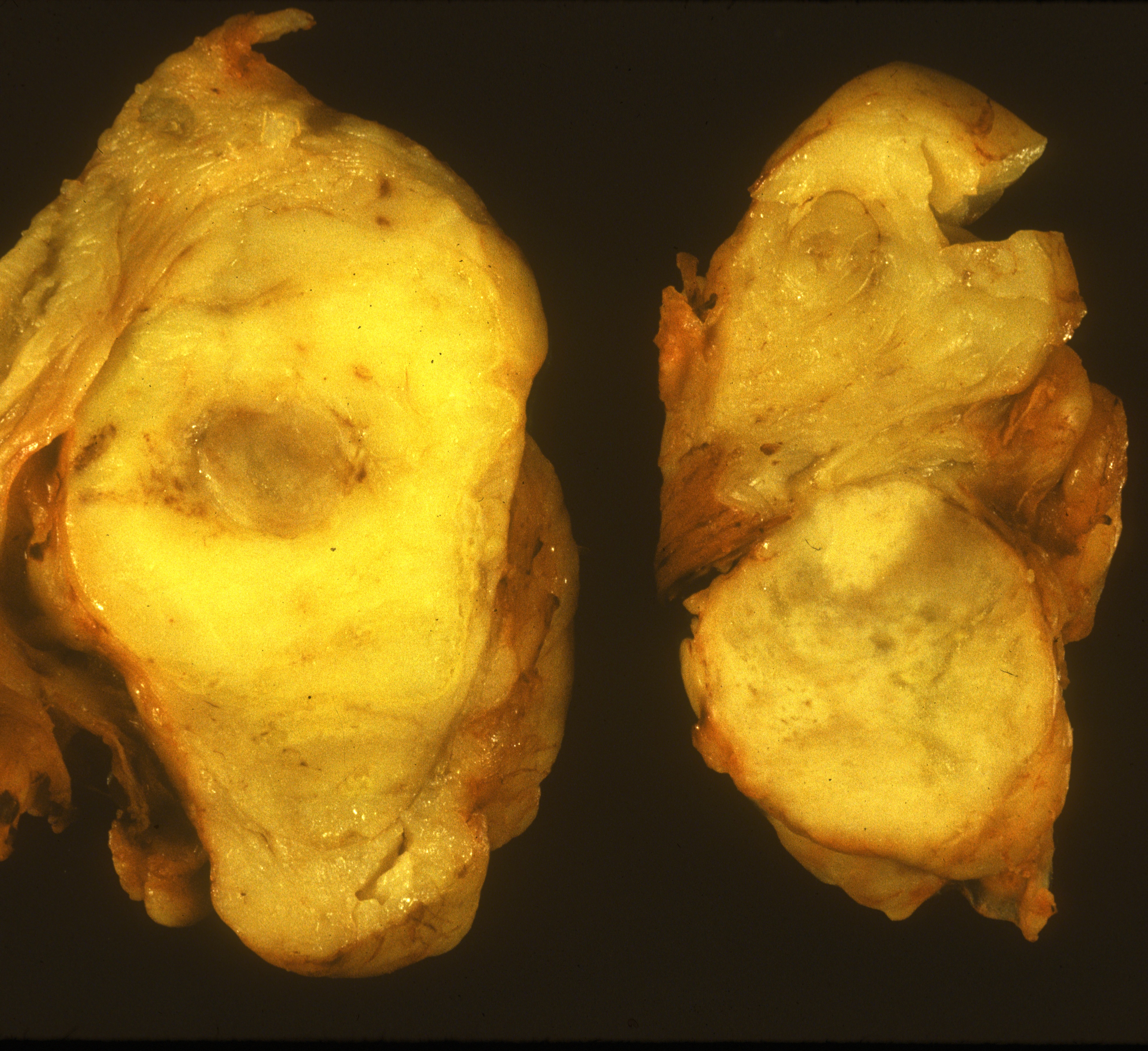 Fig. 14 Gross Pathology. A large yellow white mass is seen that resembles lipoma or a low grade liposarcoma with central fat necrosis. Gray areas correspond to non
Fig. 14 Gross Pathology. A large yellow white mass is seen that resembles lipoma or a low grade liposarcoma with central fat necrosis. Gray areas correspond to non
lipomatous tumor, the dedifferentiated area (DDLPS).
 Fig. 15
Fig. 15
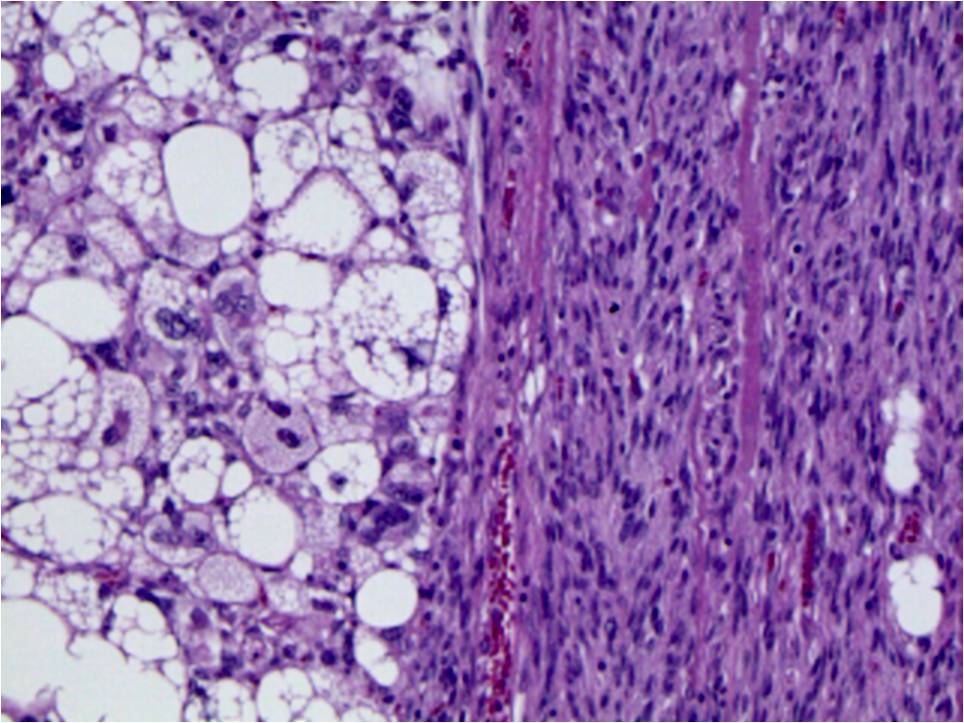 Fig. 16
Fig. 16
Fig. 15 & 16 Microscopic Pathology. Medium magnification photographs demonstrate fibrous bands with enlarged hyperchromatic spindle cells admixed with
adipose tissue corresponding to well-differentiated lipomatous tumor (Fig. 15) and sudden transition between well differentiated liposarcoma to a non-lipogenic spindle cell sarcoma (Fig. 16).
PROGNOSIS
Biological behavior
•
Up to 17% of WDLPS progress to DDLPS
•
Between 13 to 47 % of patients present with metastases.
•
DDLPS has 54-64% of overall survival
•
DDLPS has 66 to 89% of disease-specific survival
•
Location and mitotic count are the most important prognosis factors.
•
Progression to dedifferentiated LPS occurs in 17% of the retroperitoneal WDLPS and 6% for the WDLPS in the extremities.
•
Retroperitoneal WDLPS tend to progress more frequently to DDLPS.
TREATMENT
• The most reliable means of obtaining local tumor control is by wide surgical excision. In cases of positive margins re-resections should be considered
option whenever possible.
• Adjuvant radiation therapy is recommended in patients with smaller margins <10 mm after the surgical resection.
• The response rates to chemotherapy of DDLPS is still in evaluation. Some studies show that chemotherapy is not useful as a part of the treatment.
