General Information
Osteoid Osteoma is a benign osteoblastic (bone forming) tumor that is usually less than 2cm in size. It consists of a central vascularized nidus that represents the neoplastic tissue. The nidus is surrounded by normal reactive bone. It is usually a single lesion that is very painful. The nidus microscopically resembles the same type of tissue as an osteoblastoma.
Clinical Presentation
Signs/Symptoms:
- Progressive pain that is significantly relieved by aspirin or an NSAID (very rarely, less than 1%, may be painless)
- The pain is often the worst an night
- Unmyelinated nerve fibers have been demonstrated in osteoid osteomas
- Osteoid Osteomas produce high levels of PGE2 (this may be the reason why aspirin works at relieving pain, by inhibiting PGE2 production)
- Tumors next to growth plates may increase growth and cause skeletal asymmetry
- Epiphyseal lesions may cause a joint effusion and clinical picture similar to rheumatoid arthritis
- Vertebral lesions may cause a scoliosis due to muscle spasm
- Prevalence: Males more commonly affected than females ~ 3:1
Age:
- Osteoid Osteoma is most common in second decade of life
- 75%-80% of patients < 25 years
- Rarely over 30 years
Sites:
- Femoral neck most common but can occur in any bone and any site within a bone (metaphyseal, diaphyseal, epiphyseal; cortical, medullary and periosteal)
- 50% occur in long bones of lower extremities
- Most osteoid osteomas are intracortical in origin but can also occur in the medullary canal or subperiosteal
Radiographic Presentation
Plain X-Rays:
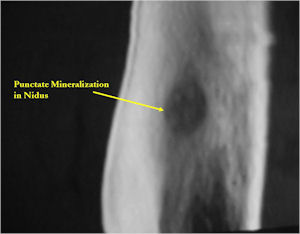
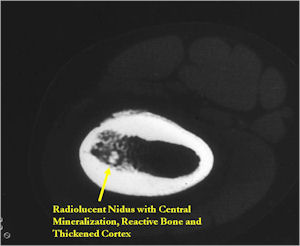
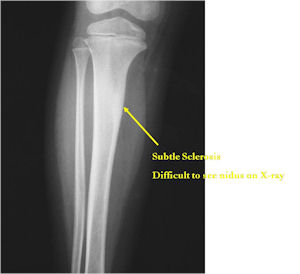
- Lucent nidus surrounded by a zone of marked sclerosis
- The nidus may demonstrate mineralization/ossification usually from the center outward that appears as a central zone of density within the nidus
- A nidus that is heavily ossified may blend in with the surrounding sclerosis and be difficult to detect on a plain x-ray.
- Periosteal bone is solid, rarely lamellated
- Cortical and subperiosteal osteoid osteomas are usually associated with much more reactive sclerosis than medullary tumors
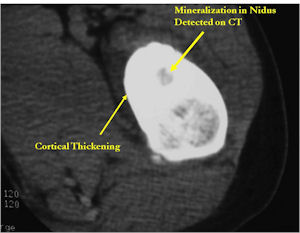
- The periosteal reaction is continuous and often appears as cortical thickening (benign appearing reaction)
- Intracapsular osteoid osteomas are difficult to identify because there is no periosteum in the intracapsular region and hence a periosteal reaction does not occur.
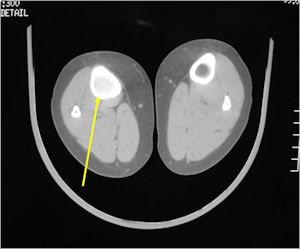
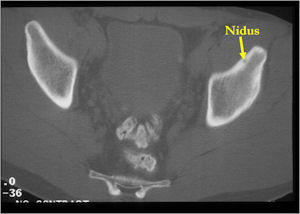
CT Scan:
- Well defined nidus with a smooth peripheral margin; +/- mineralization (CT more sensitive than XR and MRI for detecting mineralization); CT is better for detecting nidus in presence of exuberant sclerosis
- Radiographic Presentation
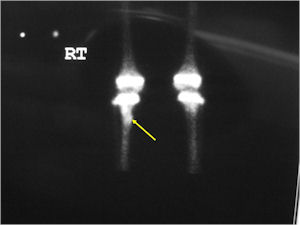
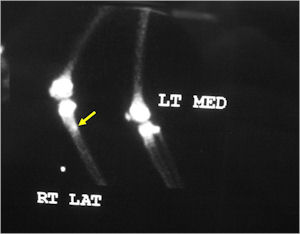
Bone Scan:
- Double Density Sign: Hot within the nidus and less intense accumulation peripherally within the sclerotic bone
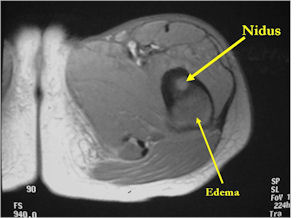
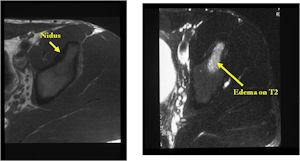
MRI:
- MRI should be performed with gadolinium if possible. The nidus should enhance with gadolinium
- An osteoid osteoma on MRI may mimic findings of a malignant tumor such as Ewing’s sarcoma or osteomyelitis because of the presence of marrow and soft tissue edema that can be extensive and make it difficult to discern a nidus.
- CT is more useful for detecting the nidus if there is extensive edema
- Osteoid Osteomas are Intermediate intensity on T1
- High intensity on T2 in areas of nidus and surrounding edema
- Reactive marrow edema may obscure the lesion on T2
- MRI is good for detecting synovitis and joint effusion with intraarticular osteoid osteomas
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
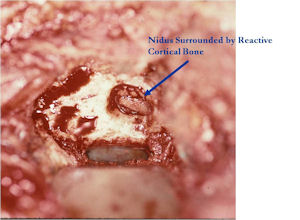
Gross Pathology
- The nidus is distinct oval/round and reddish from vascularity;
- It is well circumscribed and easily separated from surrounding bone;
- The nidus is usually less than 1 cm but may be up to 2 cm;
- The nidus may have a variable consistency depending on the extent of mineralization
- Friable, soft and granular to densely sclerotic
| Roll over the images for more information |
 |
 |
 |
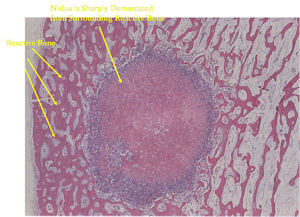
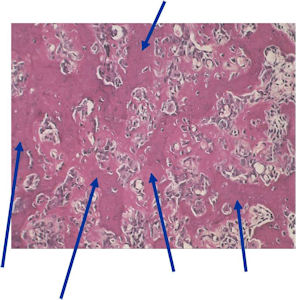
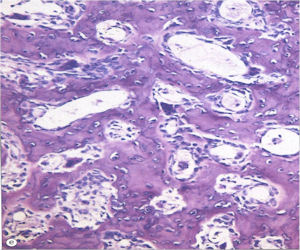
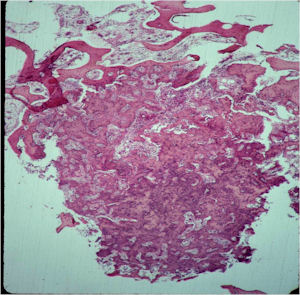
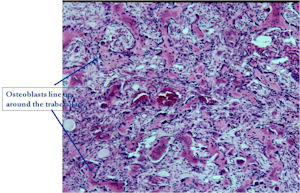
Microscopic Pathology
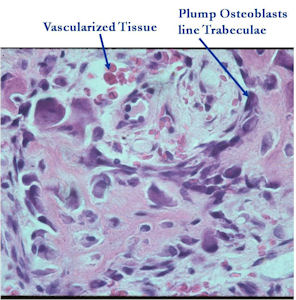
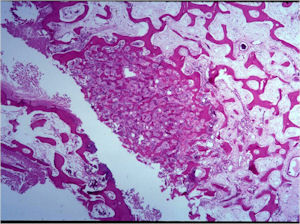
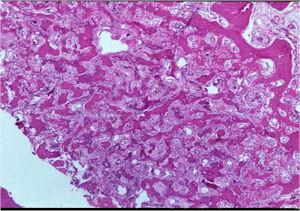
- The nidus of an osteoid osteoma consists of vascularized fibrovascular stroma and trabeculae of immature woven bone
- Nidus is sharply demarcated from surrounding reactive bone and there is an abrupt zone of transition between normal bone and the osteoid osteoma. There is no permeation of the lesion through the surrounding reactive trabeculae of bone,
- The trabeculae are uniformly lined by plump, uniform, active osteoblasts (“Osteoblastic Rimming)
- Osteoclasts may be prominent
- Mature nidus consists of more heavily calcified trabeculae of woven bone and osteoid
- No abnormal mitoses
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
Differential Diagnosis
- Differential DX of Cortical Osteoid Osteoma
- Brodie Abscess
- Stress Fracture
- Eosinophilic Granuloma
- Intracortical Hemangioma
- Bone Island
- Intracortical Osteosarcoma
- Ewing’s Sarcoma
Biological Behavior
- Osteoid osteomas exhibit limited growth potential and grow to a certain size and then stop growing;
- Some tumors may spontaneously regress;
- Osteoid osteomas that occur next to joints or intra-articularly may cause the adjacent synovium to become thickened -
- There may be chronic inflammatory cell infiltrates with lymphofollicular features in the
- synovium that can be mistaken for rheumatoid arthritis
Treatment
- Today, most osteoid osteomas are amenable to CT guided percutaneous radiofrequency ablation (RF Ablation). This is a minimally invasive technique in which the patient is put under general anesthesia and the nidus is localized under a CT scan. A needle is placed in the nidus and then the nidus is burned by means of radiofrequency waves. It is over 90% successful and there are minimal risks. Most patients notice that the pain is gone the very next day. There is little down time and most patients return to normal activities within a day or two.
- Some patients may require open surgical excision or "Burr Down Resection" of the osteoid osteoma.
Prognosis
- This is a benign tumor and there is no risk of metastasis;
- RF Ablation is effective over 90% of the time;
- Results of RF ablation are better than those reported with surgical excision and there is far less morbidity and potential complications.
Other Important Information
- May be difficult to identify nidus grossly - especially in sclerotic intracortical regions
- Tetracycline labeling is of great assistance in locating nidus
- Osteoid osteoma of the extremities may cause atrophy of nearby muscles
- If nidus is radiographically undetectable, patient may be mistakenly treated for arthritis
