Intracortical Osteosarcoma
General Information
- Intracortical osteosarcoma is an extremely rare type of osteosarcoma that arises within and is usually confined to the cortex of the bone.
- It is a high grade osteosarcoma that is confined to the cortex of a long bone
- Intracortical osteosarcoma is very rare and only a handful of cases have been reported.
- It is often initially misdiagnosed as an osteoid osteoma, bone abscess, non ossifying fibroma, osteoblastoma or adamantinoma until it is biopsied or removed
Clinical Presentation
Signs/Symptoms:
- Pain, swelling, tenderness, <1 year
Sex Predilection:
- Possible slight male predilection
Age:
Sites:
- Diaphysis of femur or tibia are the most common sites
Radiographic Presentation
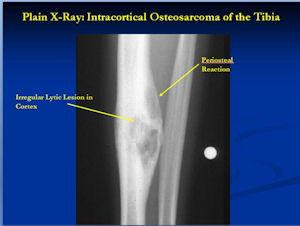
Plain Radiographs:
- Intracortical lytic lesion with surrounding sclerosis
- The junction of the lesion with the normal bone is usually irregular but sharply demarcated
- Size of lesion is usually between 1 cm to 5 cm
- Lesion may demonstrate ossification or mineralization within it
- No intramedullary or soft tissue involvement
- Minimal or no periosteal reaction or periosteal reaction may appear benign
- CT may show cortical permeation

Gross Pathology

- Intracortical, well defined tumor with very thick expanded cortex
- Irregular borders
- Thick and expanded cortex
- Tumor is grey/tan/yellow and gritty from mineralized osteoid or bone production
Microscopic Pathology
- Highly osteoblastic & sclerotic similar to a conventional osteosarcoma
- Neoplastic cells when become entrapped in osteoid may appear to normalize and have less nuclear pleomorphism and atypia
- Residual cortical bone will be entrapped by malignant cells producing osteoid (evidence of malignancy)
- There may be very small chondrosarcomatous and fibrosarcomatous foci
- Cartilage production is minimal (as opposed to a periosteal osteosarcoma)
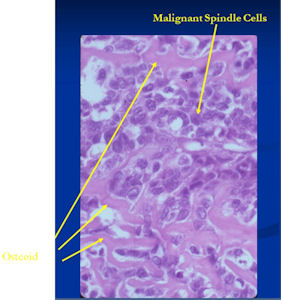
- Malignant spindle cell tumor producing osteoid
- Malignant cells have large nuclei, minimal cytoplasm, nuclear pleomorphism, mitoses
- They appear crowded and haphazard
- The osteoid is layed down in lace-like manner in between malignant cells
Differential Diagnosis
- Osteoid Osteoma
- Brodie's Abscess
- Osteoblastoma
- Nonossifying fibroma
- Eosinophillic Granuloma
- Osteofibrous Dysplasia
- Adamantinoma
Treatment
- En bloc Resection/Limb Sparing Surgery whenever feasible
- Patients treated by curettage and intralesional procedures have experienced local recurrences according to the literature
- Efficacy of chemotherapy is uncertain given the small number of cases
Prognosis
- Metastases to the lungs along with unusual sites of metastases have been reported
- Exact statistics are unavailable given the small number of patients who have been reported to develop this disease.
