General Information
- Enchondroma is a benign indolent intramedullary hyaline cartilage neoplasm
- Accounts for 10% of all benign osseous tumors
- Limited growth, most lesions are less than 5 cm in maximal dimension
- Bones grow from a cartilaginous growth plate that gradually lengthens and turns into bone as it lengthens. An enchondroma can be thought of as an island of cartilage within the bone that never transformed into normal bone. Enchondromas usually reside within the medullary canal of the bone and do not grow. In selected bones such as those of the digits of the hand or feet it may weaken the bone and predispose it to fracture.
- Enchondroma
Types:
- Solitary Enchondroma
- Multiple Enchondromas (Enchondromatosis/Ollier's Disease)
- Maffucci Syndrome (Multiple Enchondromas and Soft Tissue Hemangiomas)
Clinical Presentation
Signs/Symptoms:
- Depends on location
- Most long bone enchondromas are asymptomatic and found incidentally
- Phalangeal tumors may be painful due to stress fractures
- Prevalence:
- No clear sex predilection
Age:
- Range: Wide distribution; 5-70 years
- 60% of enchondromas are discovered in patients between 15 to 40 years of age
Sites:
- 50% involve hands and feet (mostly phalanges)
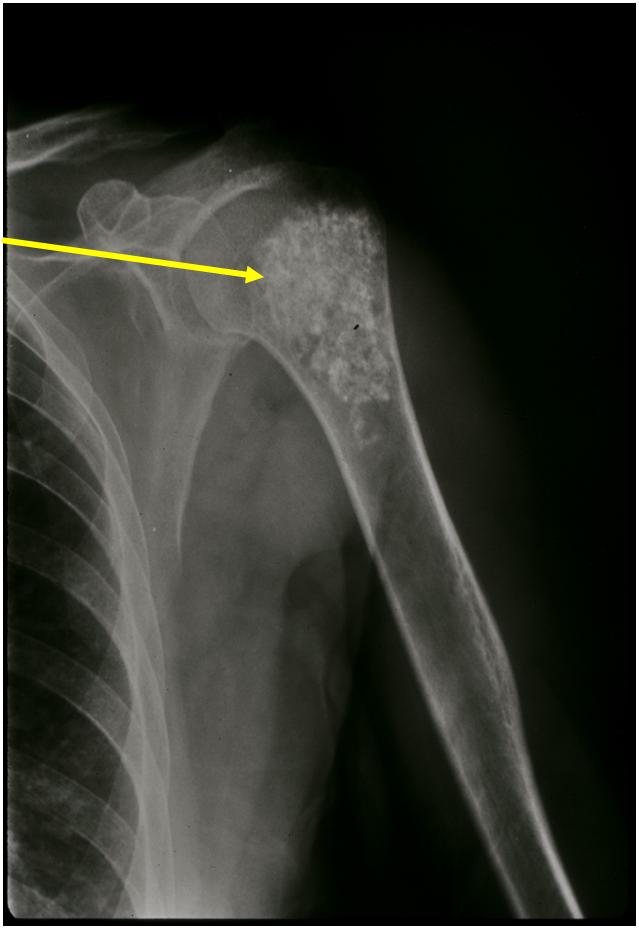
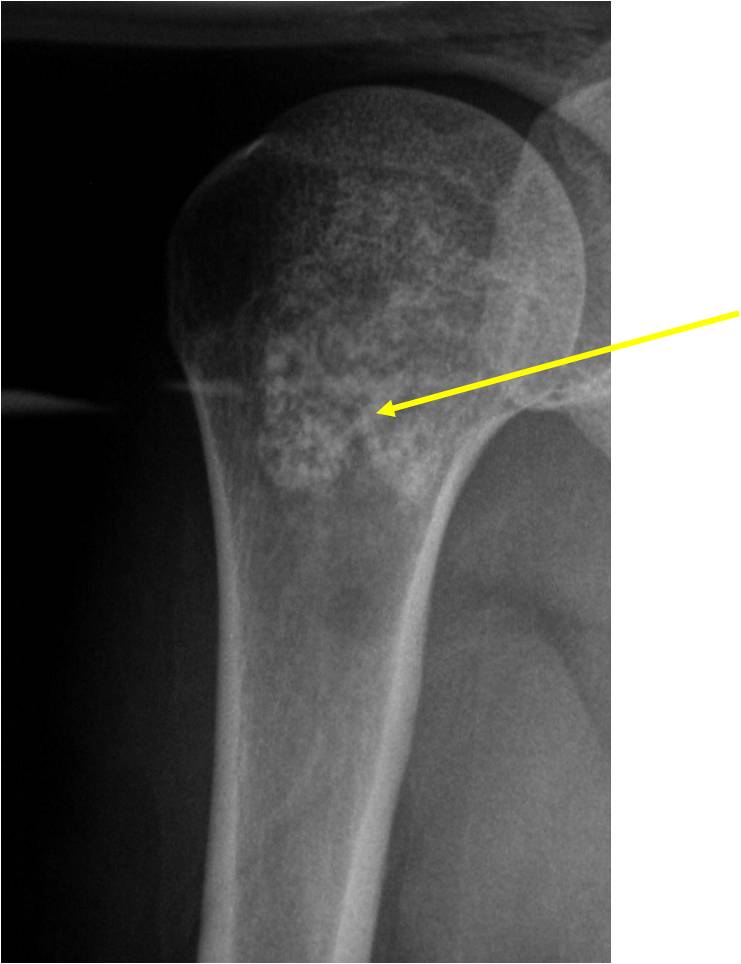
- Proximal Humerus, Femur most common long bones
- Enchondromas of the pelvis, vertebrae and ribs are uncommon
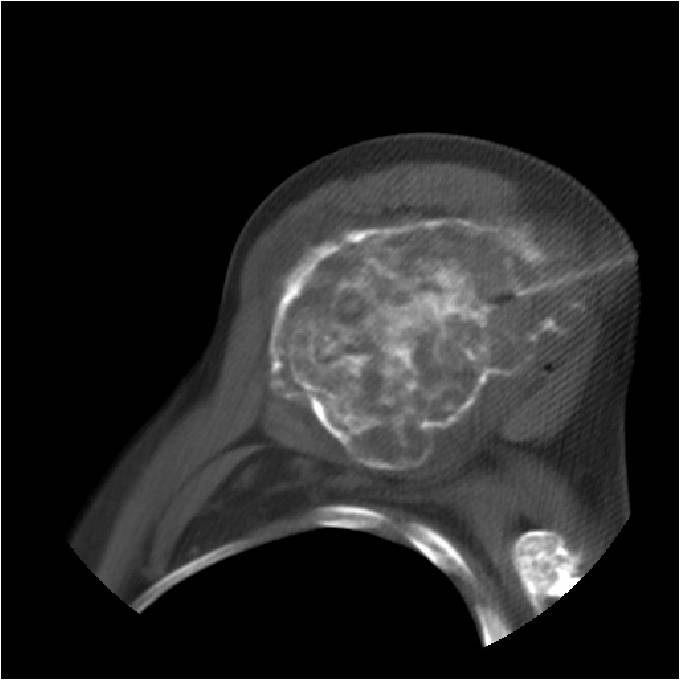
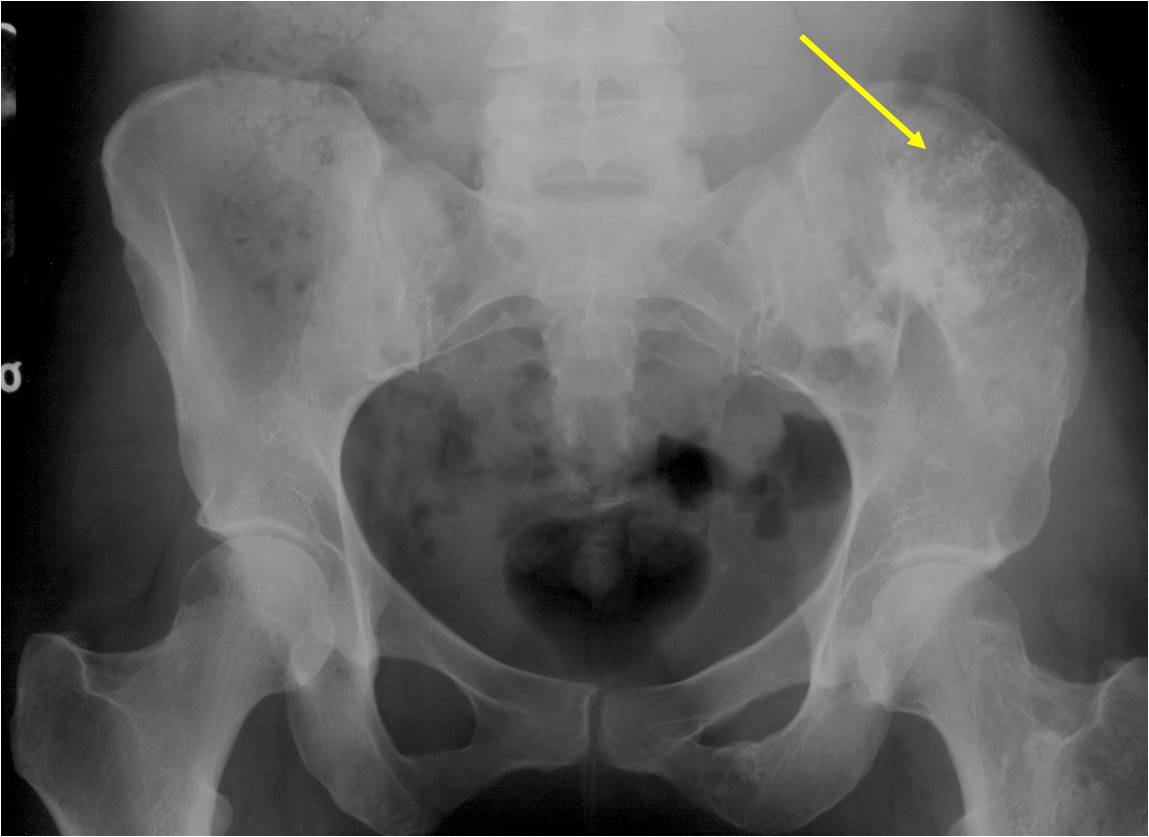
- Almost all hyaline cartilage tumors of the pelvis are considered malignant based on anatomic location no matter what the pathology shows. These tumors will ultimately grow locally and have the potential to dedifferentiate or change into a higher grade chondrosarcoma.
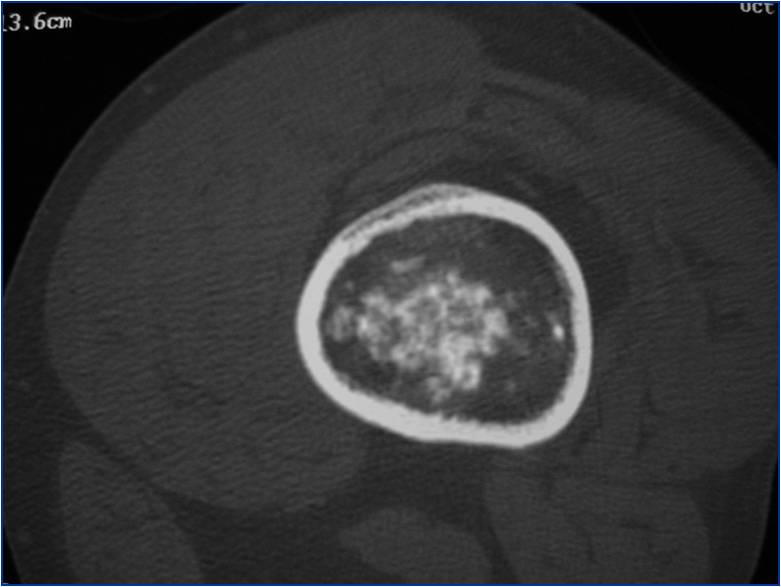
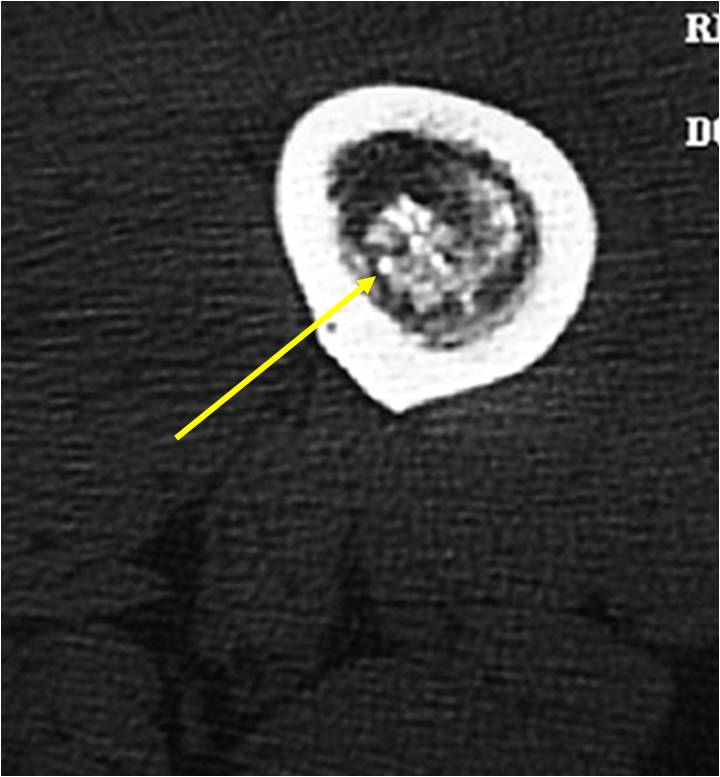
Radiographic Presentation
- Localized, radiolucent defect usually with punctate calcifications
- Calcifications are typical but not always present
- Matrix may demonstrate various degrees of calcification
- Calcifications are stippled, punctate, popcorn like calcifications and "Ring and Arc" calcifications
- Cartilage tumors grow in a lobular manner. The perimeters of the lobules undergo
- enchondral ossification that may calcify. If the entire perimeter of the lobule calcifies it appears
- radiographically as a "Ring". If a portion of the perimeter of a lobule calcifies it forms an "Arc" on
- an X-ray.
- May be located centrally or eccentrically
- Grows eccentrically or concentrically (phalanges)
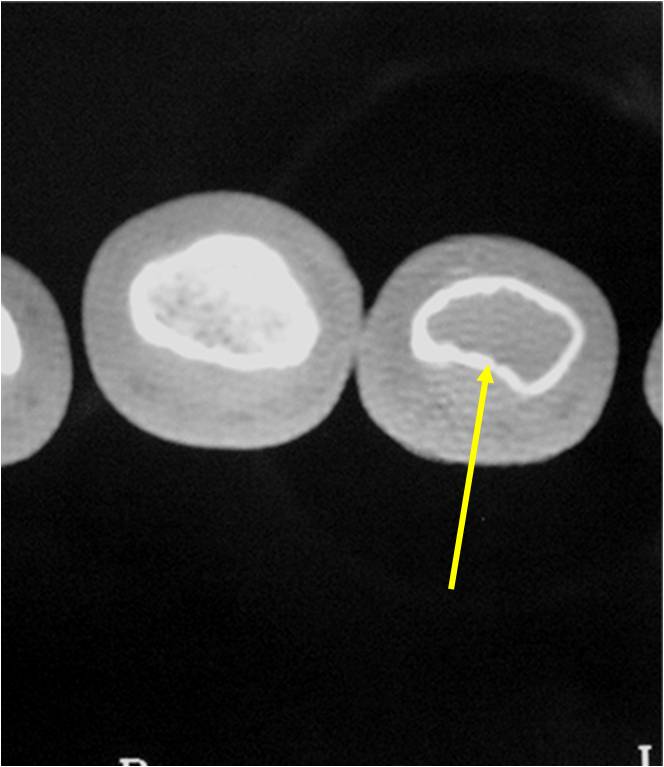
- Cortex may be scalloped and thinned in the phalanges
- MRI is better to see noncalcified chondroid lesions and the full extent of lesions
- Most commonly found in metaphysis
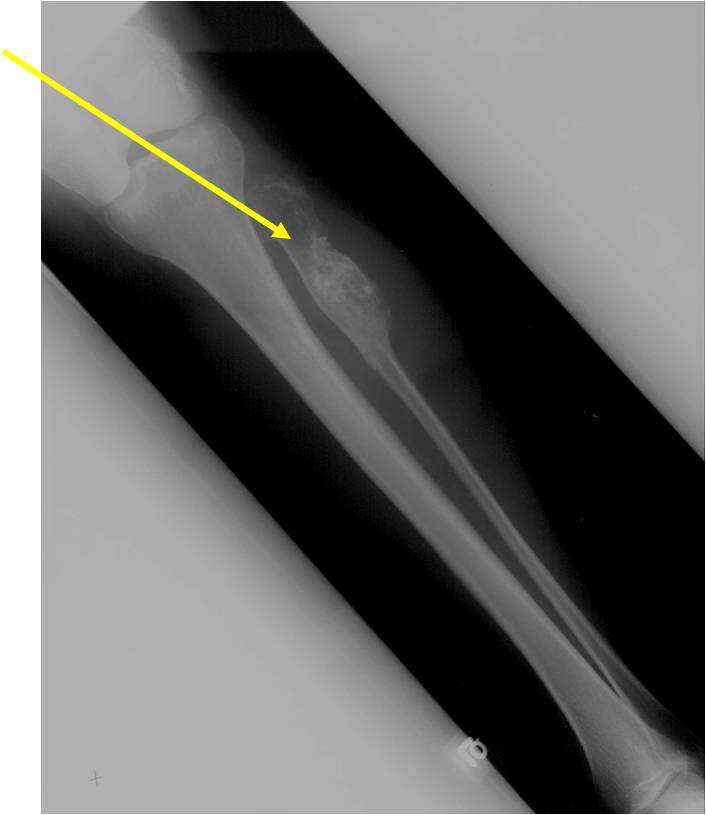
Plain X-Ray:
- Geographic lytic lesion
- Central often metaphyseal in long bones
- Expansile remodeling with thinned cortex
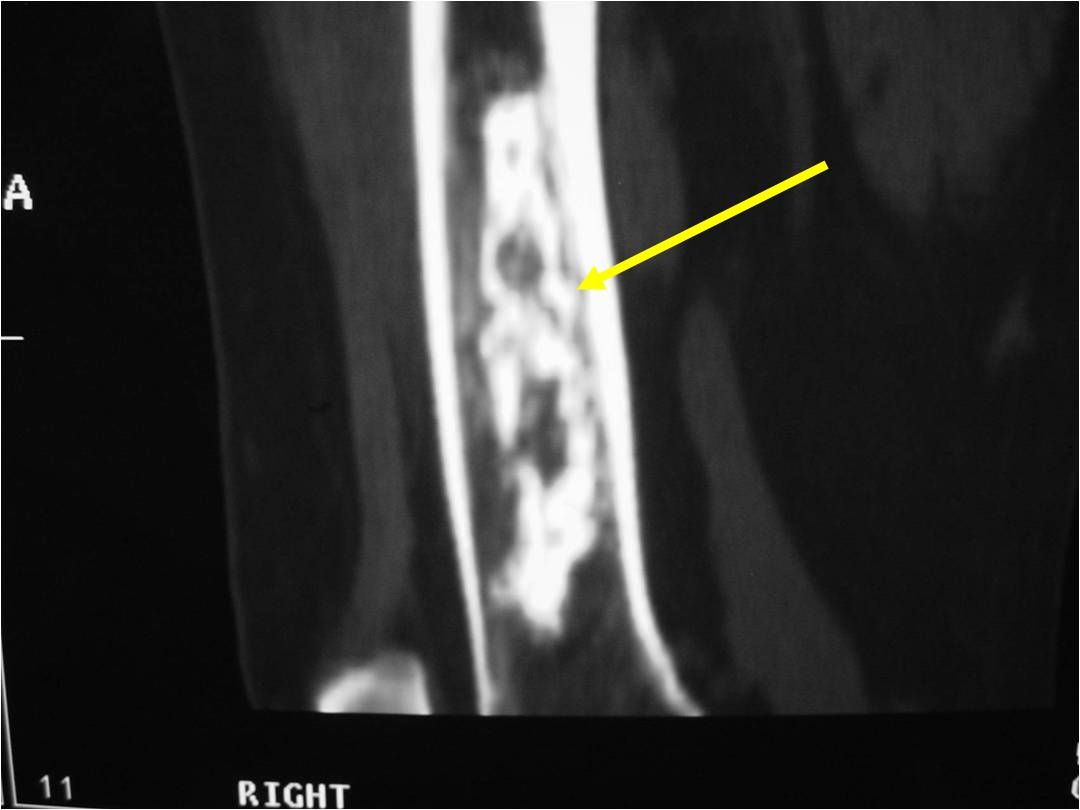
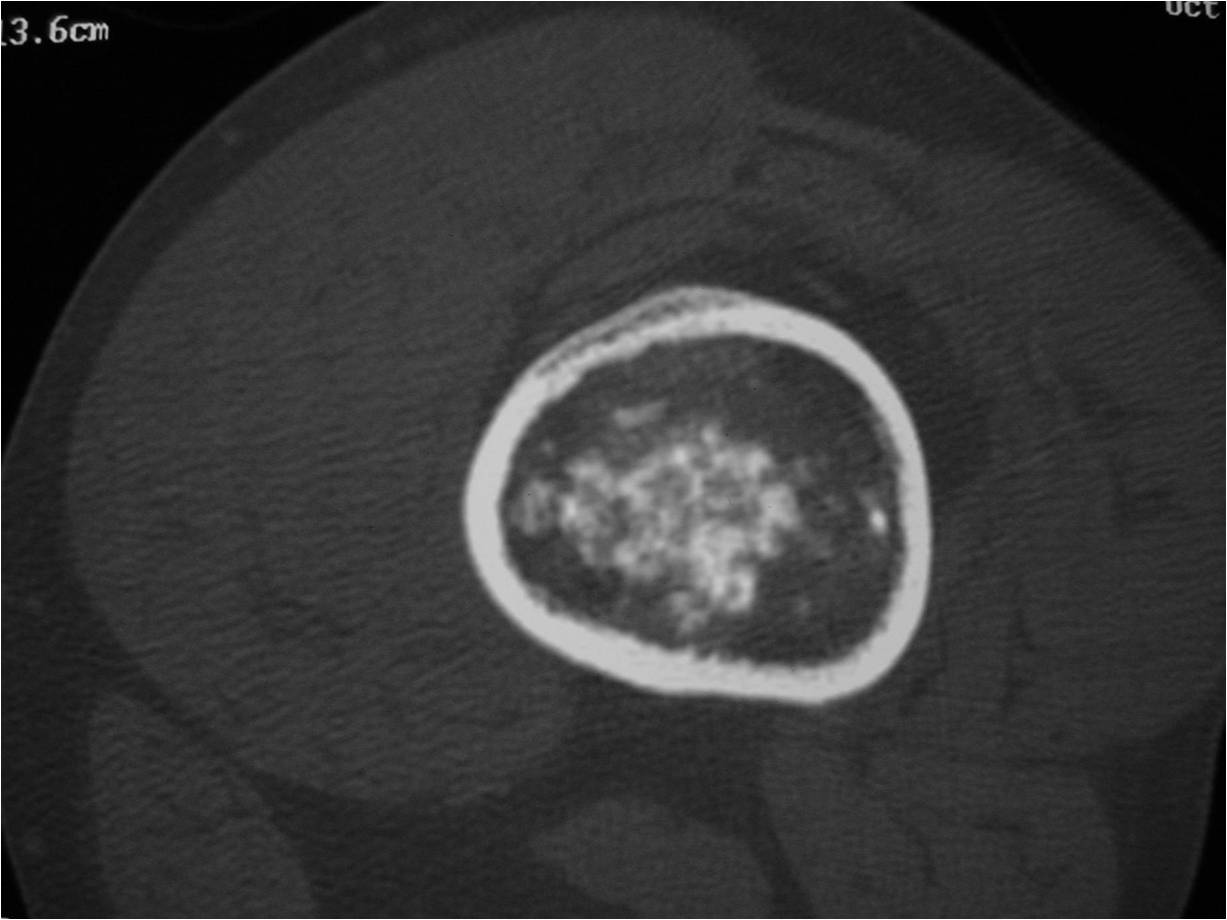
- Chondroid matrix with calcifications in majority of tumors
- Approximately 20% have limited or no calcifications
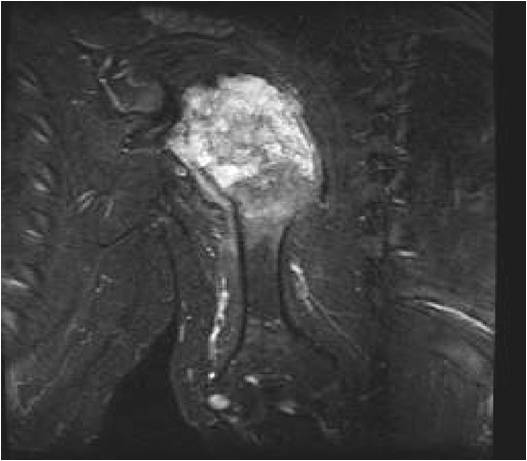
- MRI
- Lobulated margin
- Marked increased intensity long TR images
- Calcified chondroid - low intensity all sequences
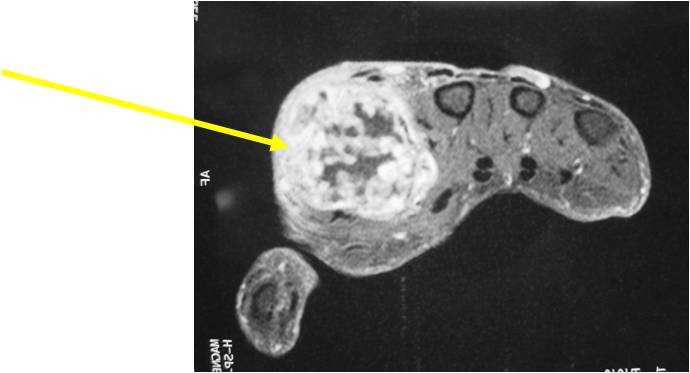
MRI:
- Lobulated margin (Lobular Growth Pattern)
- T1 Weighted Images: Intermediate Signal Intensity
- Calcifications will be low signal
- T2 Weighted Images: High Signal Intensity
- High water content shows as high signal on T2 weighted images
- Calcifications will be low signal
- Marked increased intensity long TR images
- Calcified chondroid - low intensity all sequences
- There should never be any cortical destruction nor a soft tissue component. If this exists then the tumor must be a chondrosarcoma.
- Endosteal scalloping and cortical expansion is acceptable for phalangeal tumors. In most benign long bone cartilage tumors there is minimal endosteal scalloping but there should be no cortical expansion nor thickening. There should be no cortical destruction and no soft tissue component associated with an enchondroma. Cortical destruction, periosteal thickening, cortical expansion and a soft tissue component indicates a chondrosarcoma of the long bone.
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
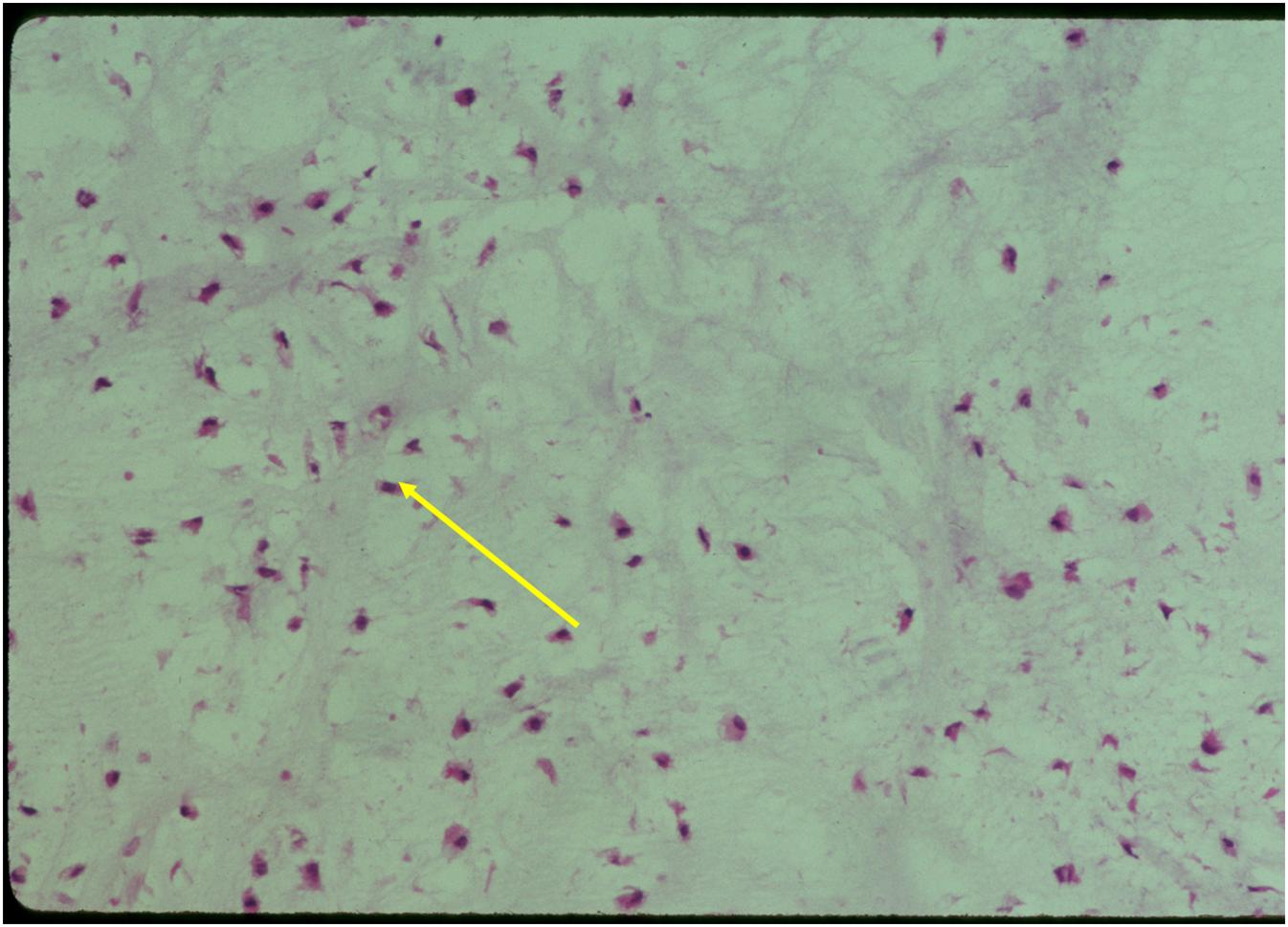
Pathology
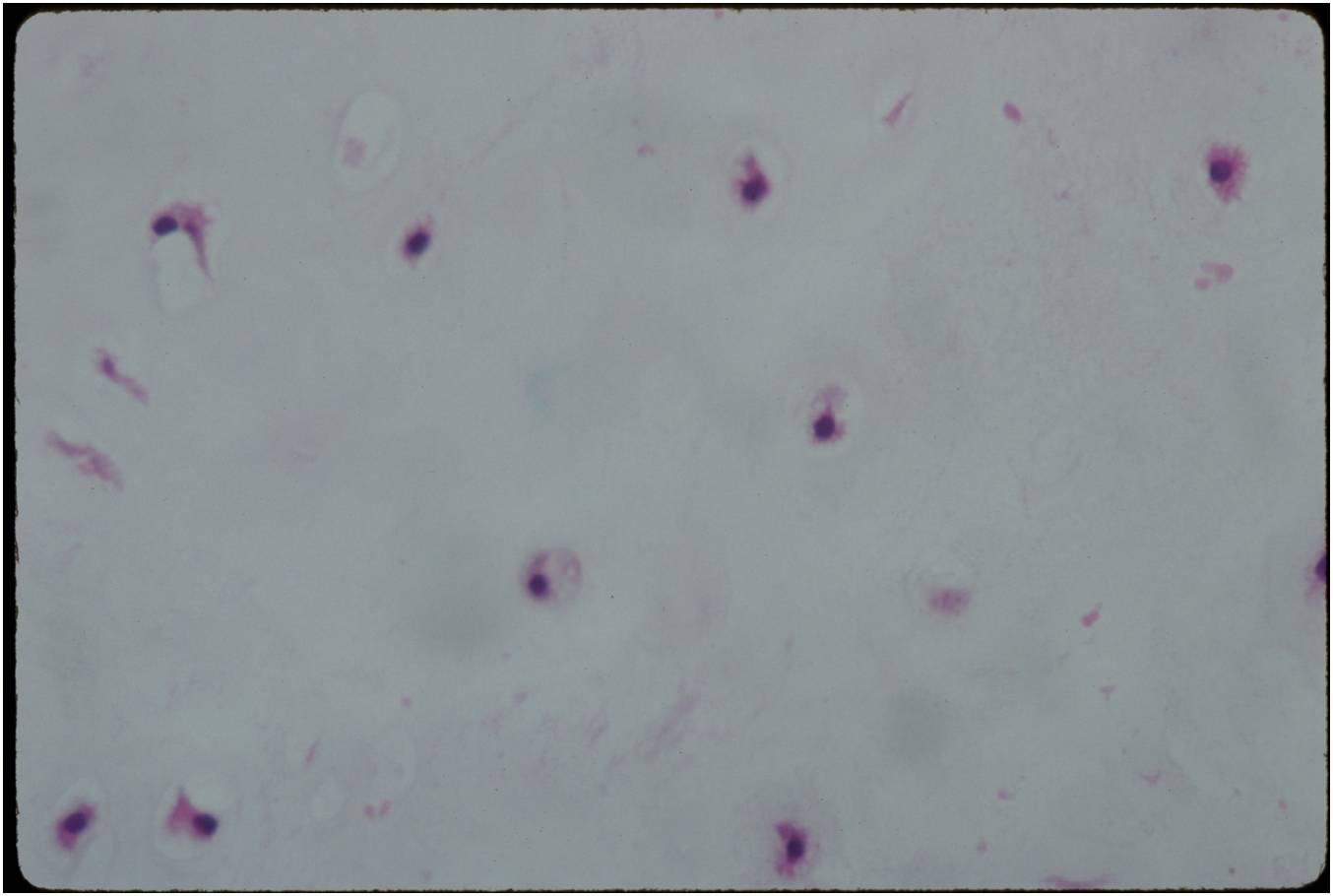
- Rests of hyaline cartilage with a lobular growth pattern
- Cells are within lacunae
- Hypocellular with cells spaced apart separated by matrix
- Cells have small nuclei and are similar size and shape (no pleomorphism)
- No mitotic figures
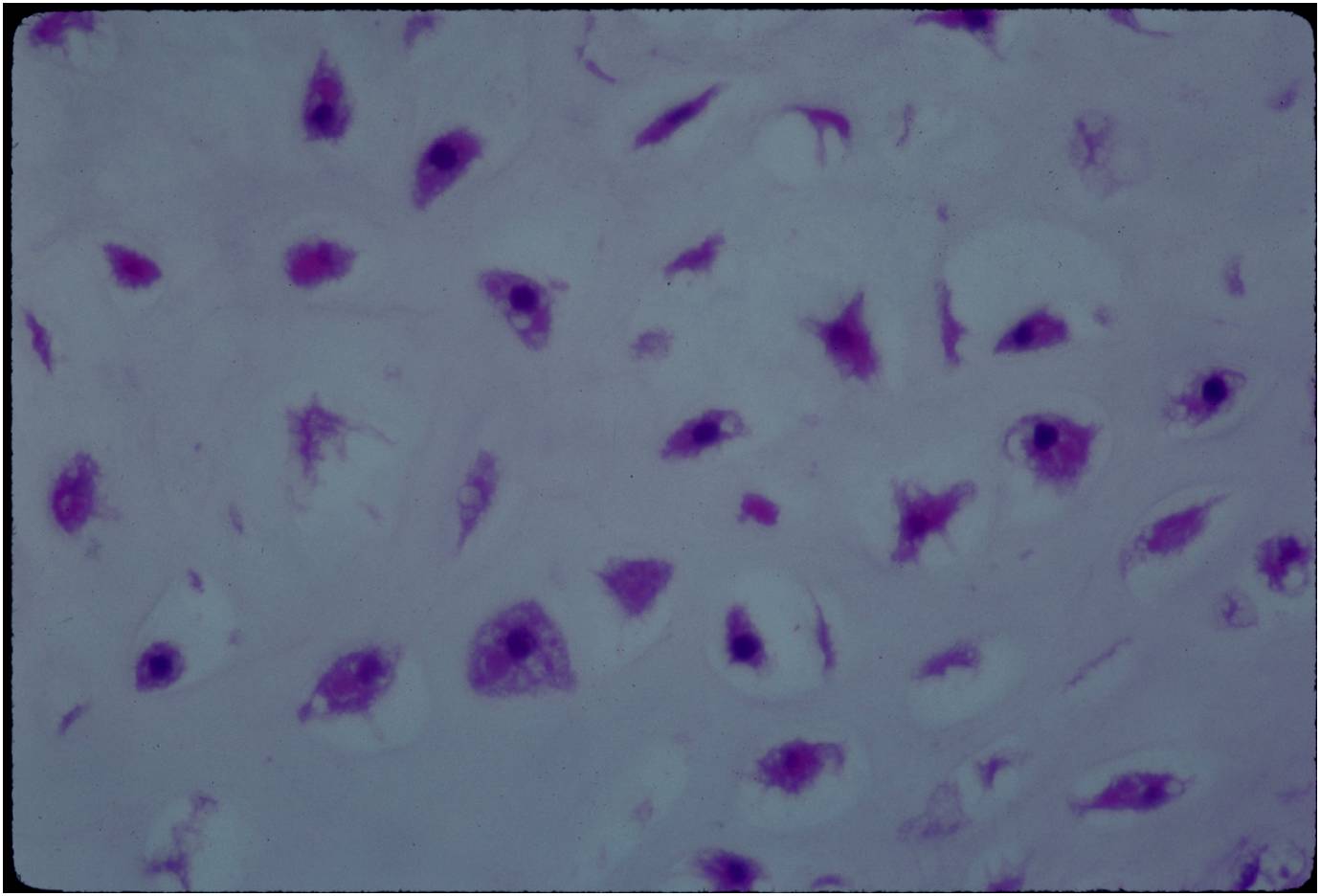
- The matrix has a ground glass basophilic appearance
- The matrix contains glycosaminoglycans that attract fluid/water and gives it a bsophilic appearance and show as high signal intensity on T2 weighted MRI
- The collagen of the matrix is organized in a manner such that the refractile index under a microscope gives a ground glass appearance to the matrix. One can not visualize the actual collagen fibers.
- Hyaline cartilage often with myxoid areas
- Variable amorphous calcification and enchondral ossification
- May cause mild expansile remodeling of bone and cortical thinning
Gross Pathology
- Fragments of enchondroma after curettage are bluish white and glistening hyaline cartilage
- There may be yellow calcified foci
- Cartilage grows in a lobular manner and hence in a completely resected specimen there will be local lobules of mature cartilage
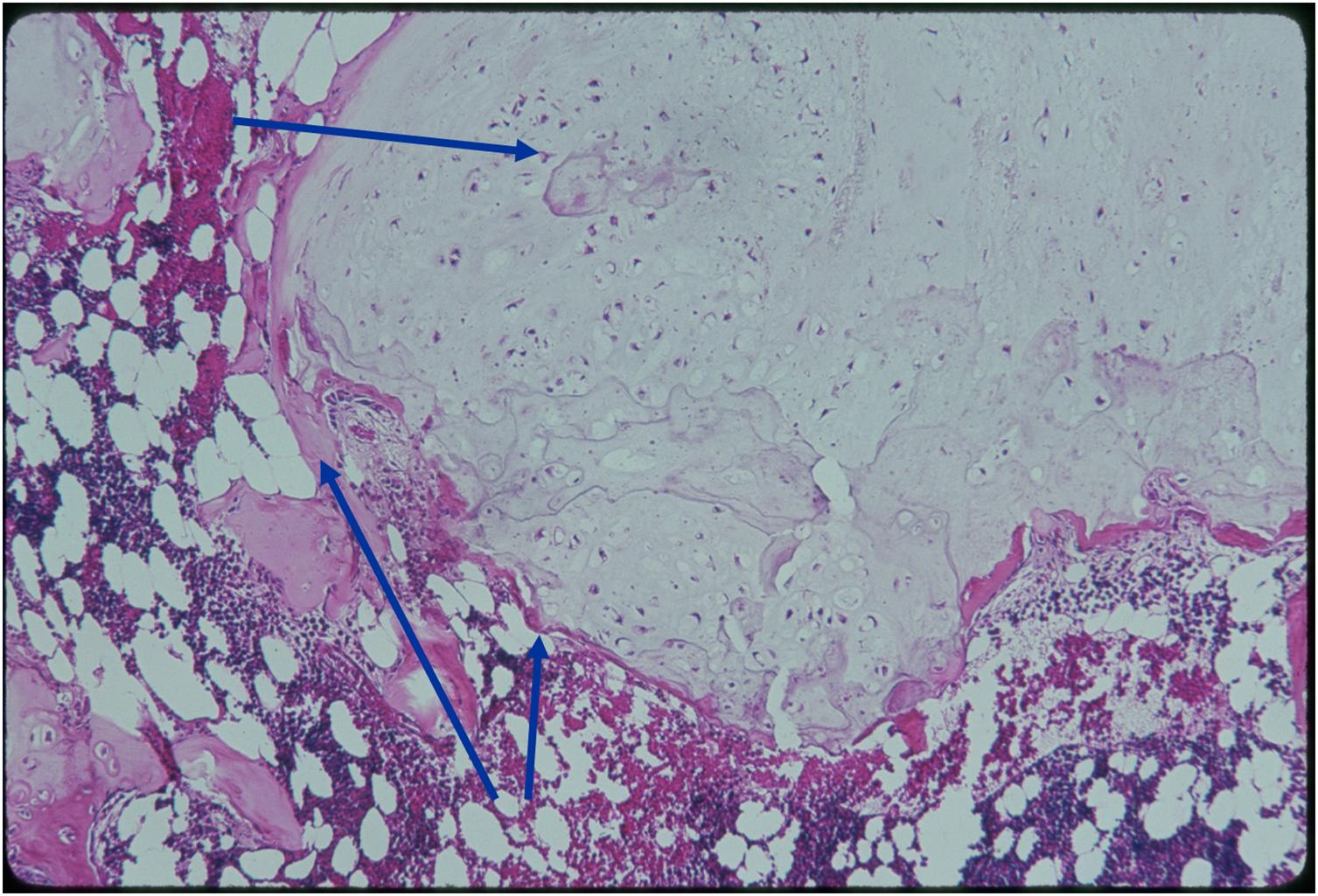
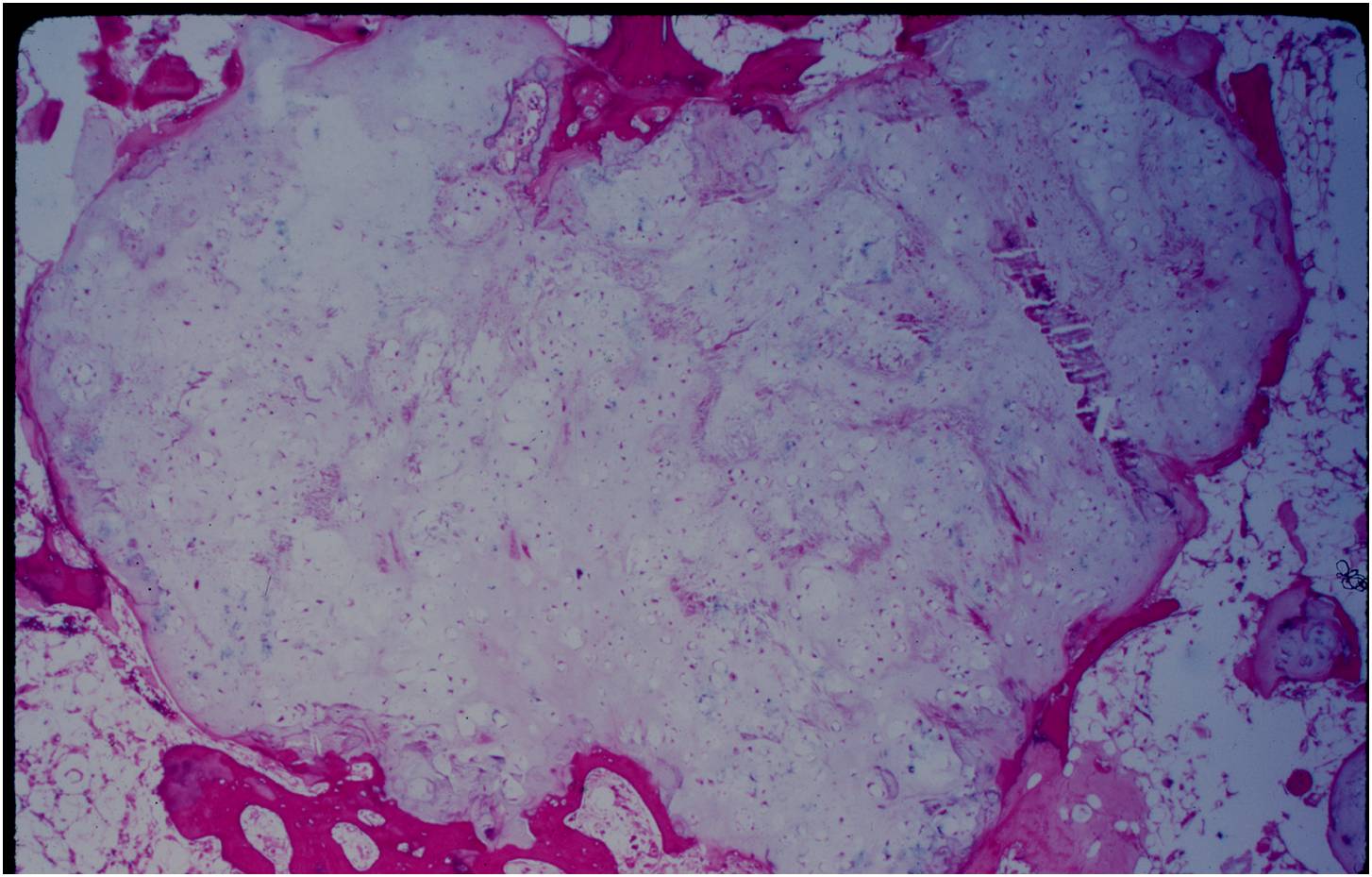
Microscopic Pathology
- Enchondromas are well defined lesions with cartilage arranged in lobules that are separated by fibrovascular septa
- Enchondral ossification may occur around periphery of lobules and when calcified appear as "Rings and Arcs" on X-rays
- Cells are in lacunae and have small dark nuclei
- Low cell count, cells appear bland with few chondrocytes and are similar size and shape
- Although some enchondromas may have areas that are hypercellular and may have two or three cells within a lacunae
- No entrapment or destruction of trabeculae
- There should be no myxoid change in long bone lesions (there is occasional myxoid change in enchondromas of the digits)
- Presence of myxoid change is sign of malignancy
- Enchondromas of digits can have hypercellularity, bi and trinucleated cells and myxoid change and still be considered benign
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
Differential Diagnosis
- The main differential is with a low grade (Grade 1) chondrosarcoma
- Can be very difficult to differentiate from a Grade 1 Chondrosarcoma from an enchondroma based on histology
- It is easy to differentiate from a grade 2 or 3 chondrosarcoma by means of histology which are hypercellular, pleomorphic and demonstrate mitotic figures
- Radiographs and clinical history are important for differentiation
- Biopsies are not useful for differentiating an enchondroma from a low grade chondrosarcoma
- Features consistent with chondrosarcoma
- Pain attributable to lesion
- Age greater than 50
- Cortical destruction and a soft tissue mass
- Periosteal reaction and thickening
- Endosteal erosion>2/3 cortical thickness on a CT scan
- Size greater than 5 cm
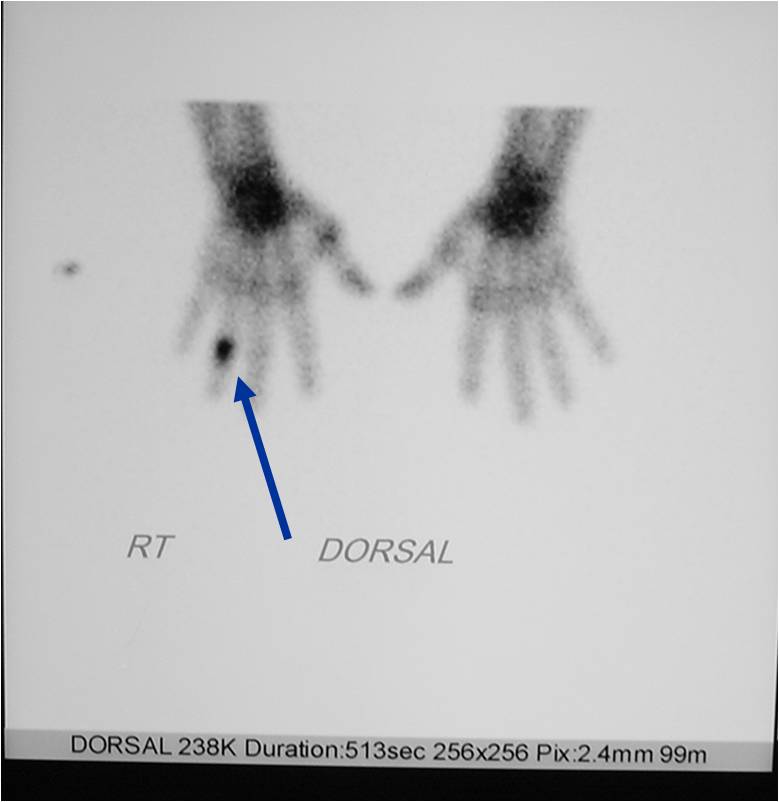
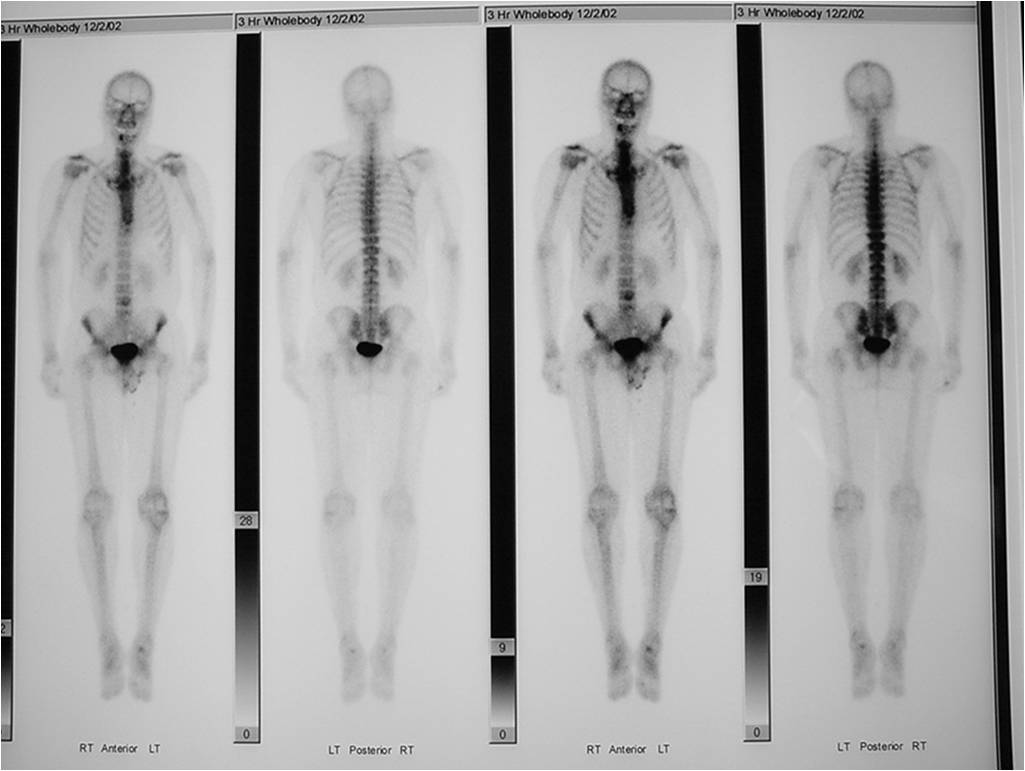
- Bone Scan: Lesion that is hotter than ASIS
Treatment
- Enchondromas are benign, indolent (not growing) tumors
- Indications for surgery:
- Digits: Impending or actual pathological fracture
- Intralesional curettage and bone graft or cement
- Long bones: Rare to fracture—usually observe
- If grows it is considered chondrosarcoma and would recommend surgery accordingly
Prognosis
- Recurrence rate following curettage is <5%
- Recurrence of an enchondroma suggests malignancy
- There are rare cases where enchondromas can dedifferentiate into a chondrosarcoma or dedifferentiated chondrosarcoma (low grade chondrosarcoma with an osteosarcoma, fibrosarcoma or malignant fibrous histiocytoma arising adjacent to it)
Enchondromatosis
- (Multiple Enchondromas/Ollier Disease
- Enchondromatosis is a rare disorder that is not hereditary in which the patient is afflicted with multiple intraosseous cartilaginous tumors or enchondromas.
Clinical Data:
- Mild male predilection
- Present in childhood
- Usually affects the extremities
- Variable severity
- May be predominantly unilateral or affect a single extremity/limb
- Affected limb is often shortened and deformed and angulated
- May become stable at puberty
- Higher risk of malignant transformation to chondrosarcoma (5-50%) as opposed to an isolated enchondroma
- Marked skeletal deformity
- Not hereditary
Enchondromas in enchondromatosis may involve the metaphysis, diaphysis, epiphysis and articular cartilage
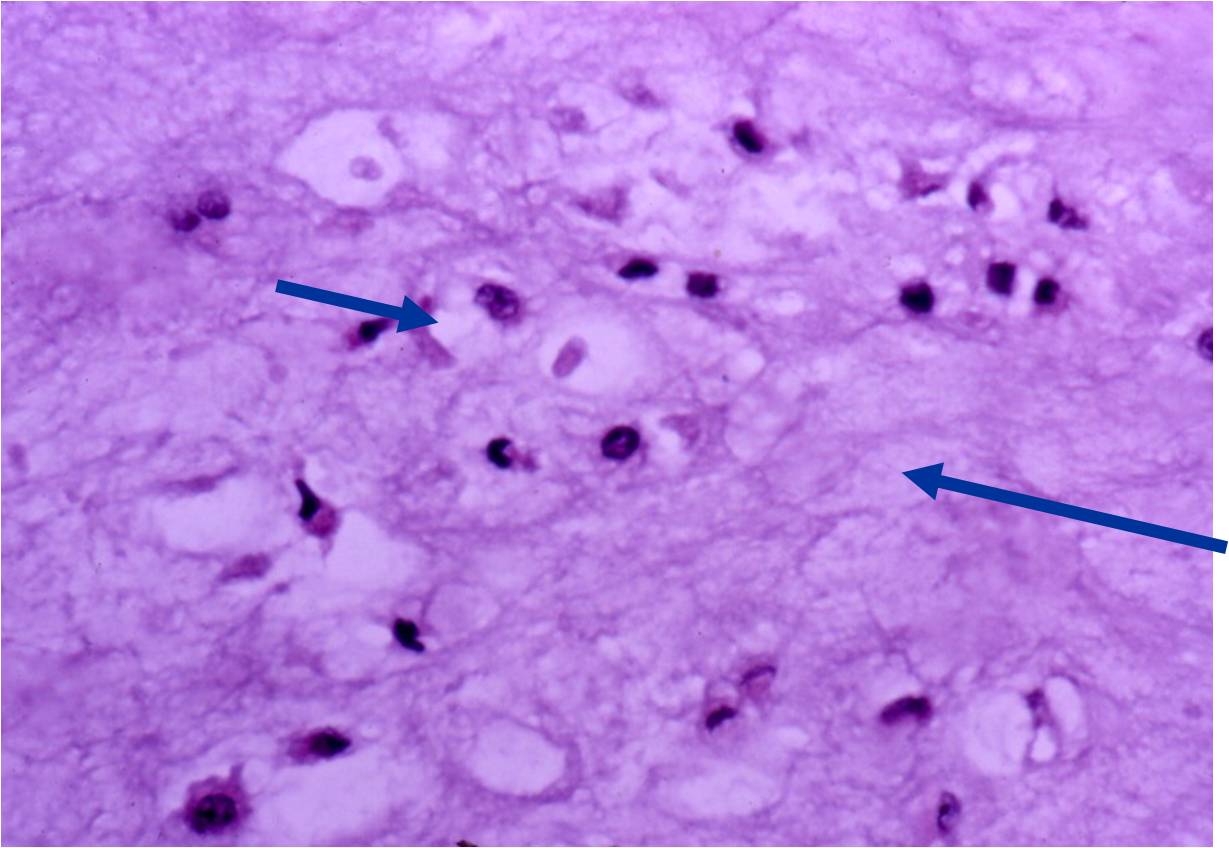
Microscopic Pathology
- Hypercellular with large number of binucleated chondrocytes
- Higher degree of cellularity and atypia compared to isolated enchondroma
- Diagnosis of benign cartilage from a chondrosarcoma in setting of enchondromatosis is very difficult. Necrosis, myxoid change and radiographic studies demonstrating cortical destruction or a soft tissue mass are consistent with a chondrosarcoma
- Chondrosarcoma arising in enchondromatosis
- Patients with enchondromatosis are predisposed to developing chondrosarcomas and reports have documented up to a 50% risk for developing a chondrosarcoma over a lifetime.
- Usually there is pain, cortical destruction and an enlarging mass
- Most are low grade chondrosarcomas but dedifferentiated chondrosarcomas can also occur
- Most patients are between the ages of 30-60 when they develop a secondary chondrosarcoma
- The most common sites to undergo malignant change are the scapula, rib cage and pelvis
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
Chondrosarcoma arising in enchondromatosis - The prognosis for patients who develop a chondrosarcoma in setting of enchondromatosis is the same as a patient who develops a chondrosarcoma without a pre-existing condition. Low grade chondrosarcomas are associated with a good prognosis and mot patients are cured with surgical removal. Patients who develop a dedifferentiated chondrosarcoma have a high risk of developing metastases, dismal prognosis and high mortality rate.
Maffucci Syndrome
- (Described in 1881 by Maffucci as enchondromatosis with hemangiomas)
Clinical Data:
- Very rare; Nonhereditary
- Multiple Enchondromas
- Cavernous Hemangiomas anywhere in skin and subcutaneous tissues of body
- May be unilateral or bilateral, may be only a few or many
- Phleboliths (calcifications) usually seen in hemangiomas on X-ray
- Mild male predilection
- Hands and feet greatest involvement
- Complications of hemangiomas
- Malignant Transformation: Chondrosarcoma (15-20%) Vascular Sarcoma (3-5%) Ovarian Malignancy Glioma and Carcinoma Unrelated to bone or soft tissue
Imaging characteristics:
- Lesions seen in infancy
- Typical enchondromas
- Geographic IA-IIB with expansion
- Lytic columns from epiphyseal plate
- Chondroid matrix calcification
- Growth disturbance and bowing
- Enchondroma growth slows after growth plate closure
- Maffucci: Soft tissue mass/hemangiomas with phleboliths
- Chondrosarcomatous transformation
- New bone destruction
- New periosteal reaction
- Disorganized or destroyed matrix calcification
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
