GENERAL INFORMATION
Desmoplastic fibroma is a benign but aggressive tumor composed of fibroblasts and myoblasts in heavily collagenized stroma. It's a very rare tumor with slow growth and produces collagen. It characterized also by aggressive intramedullary proliferation of myofibroblasts. This tumor grows locally in bone in an aggressive manner and destroys the bone. It has significant potential for local recurrence.
CLINICAL DATA
• Myofibroblasts are well-differentiated within a dense collagen matrix
•
Rare, represents 0.1% of all bone tumors
•
Microscopically identical to soft tissue fibromatosis
•
Fibrous dysplasia may be incorrectly diagnosed as Desmoplastic Fibroma
Differential Diagnosis
• Low grade fibrosarcoma
• Giant cell tumor
• Non-ossifying fibroma
• UBC
• Chondromyxoid fibroma
• Fibrous dysplasia
CLINICAL PRESENTATION
Signs/Symptoms
• Pain and swelling up to 3 years duration
• Associated with pain and deformity in cases of pathologic fracture
Prevalence
• No discernable predilection for any race/sex
Age
• Range 20 months to 70 years
• Rises mostly in second decade of life (46%)
• 78% cases present before age of 40 years.
Sites
• Craniofacial bones
• Mandible most frequent
• Long bones-----metaphyseal femur, tibia, humerus
RADIOGRAPHIC PRESENTATION
Plain x-ray (Fig. 1-2)
• Well-defined, lucent and expansile
• Possible cortical degradation
• Possible involvement of soft tissue
• More destructive, aggressive growth
• Shown by less-defined borders
• Pathologic fracture may occur
• Described as moth eaten
CT (Fig. 3)
• Useful to demonstrate cortical destruction
MRI (Fig. 4-5)
•
Ideal to describe soft tissue involvement
• Sequences often follow that of fibrous tissue with low signal on T1 weighted and T 2 weighted images
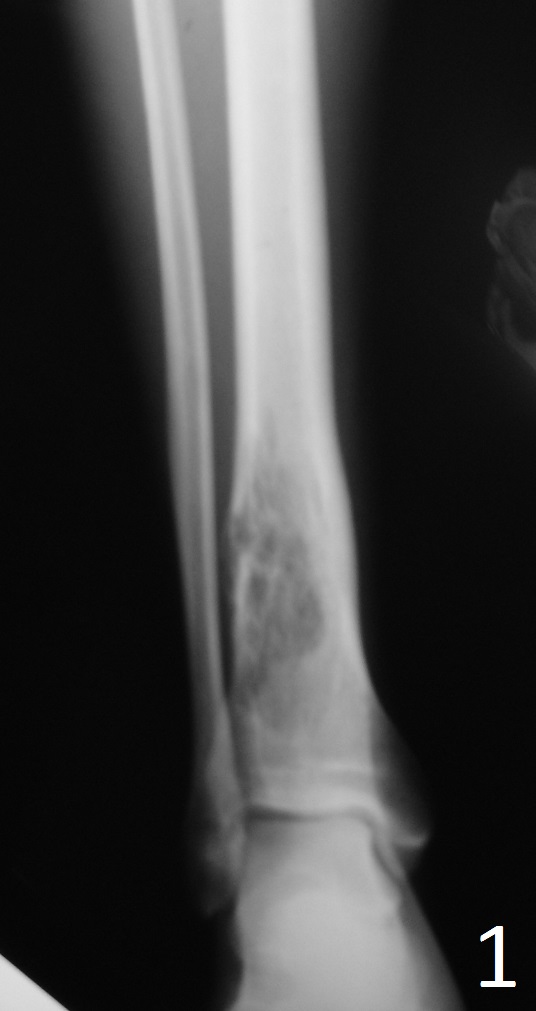 Fig. 1: AP and Lat (Fig. 2) Xray of tibia-fibula show a lucent distal tibia lytic lesion. Desmoplastic fibroma of bone often has thickened internal trabeculations and arises within the ceter of medullary canal.
Fig. 1: AP and Lat (Fig. 2) Xray of tibia-fibula show a lucent distal tibia lytic lesion. Desmoplastic fibroma of bone often has thickened internal trabeculations and arises within the ceter of medullary canal.

Fig. 2
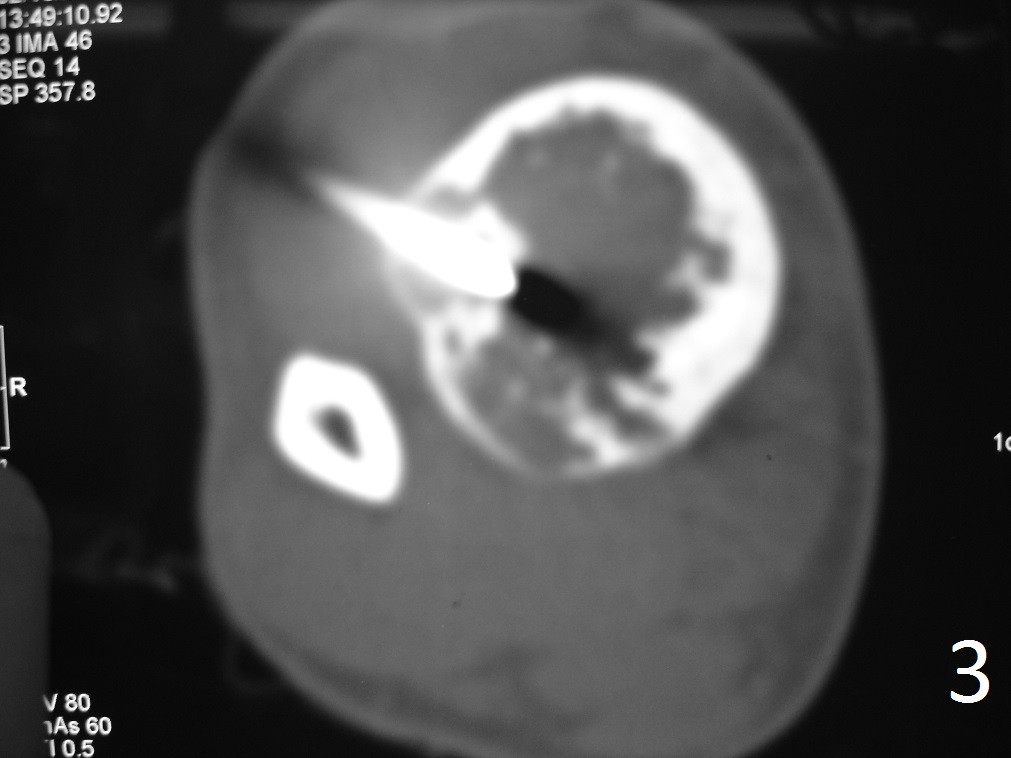
Fig. 3: Axial CT reconstruction of lower extremity, shows a lytic lesion with posterior cortical destruction during CT guided biopsy.
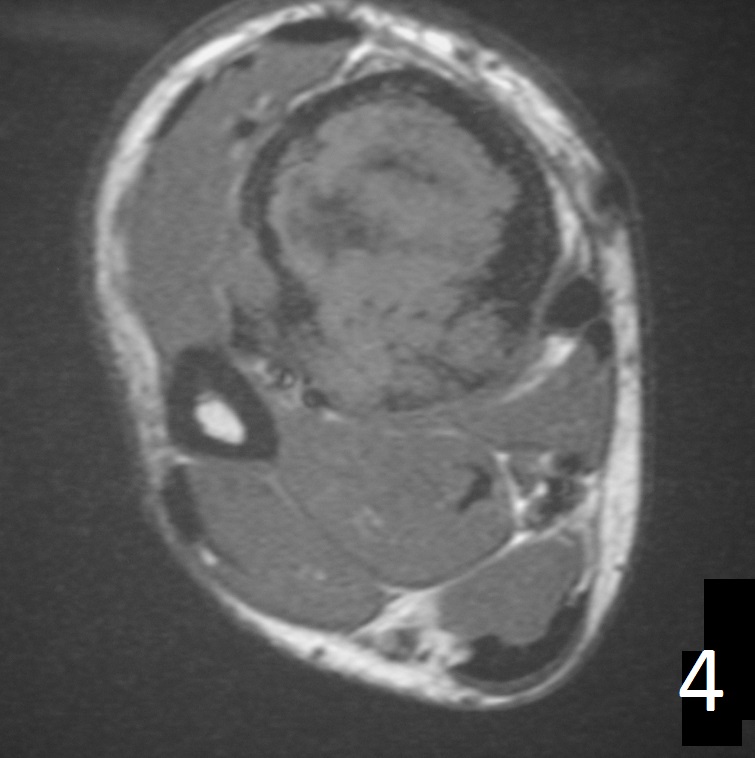
Fig. 4
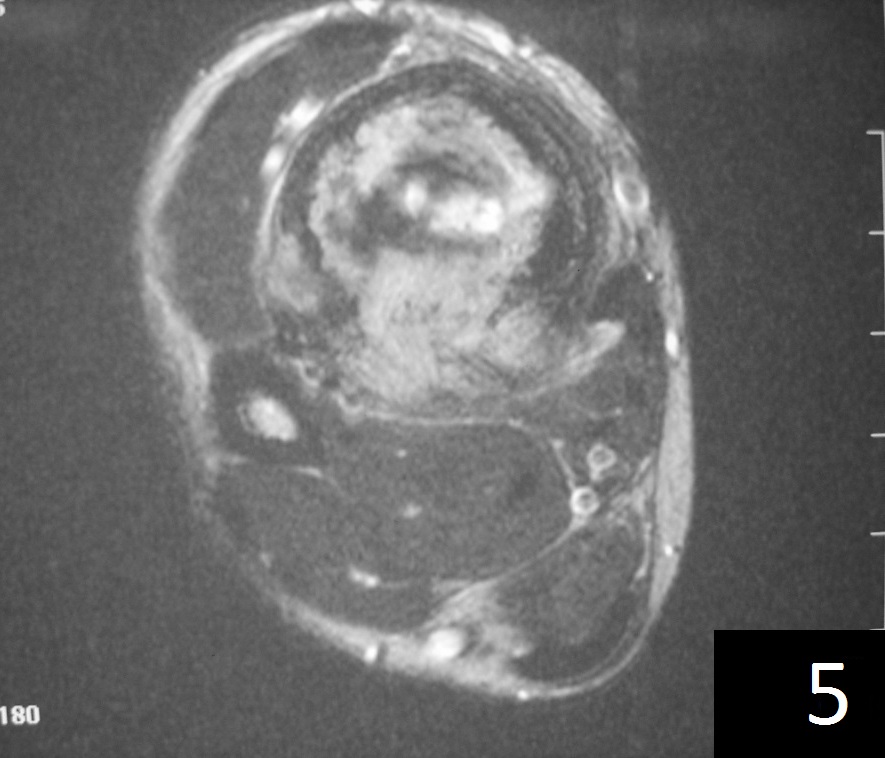
Fig. 5
Fig. 4-5: Axial MRI of leg demonstrates a tibia lesion with cortical destruction and soft tissue involvement.
PATHOLOGY
Gross
•
Lesion ranges from 3 cm to 10 cm in size
• Grey/white, solid, and fibrous
• Resemble desmoid soft tissue tumors
Microscopic
•
Lesion consists of spindle-shaped fibroblasts with dense collagen
• Irregular cellular consistency within lesion
• Low mitotic activity, nucleoli are absent
• Difficult to differentiate from secondary reactive fibrosis
• Entrapped remnants of bone are often present
PROGNOSIS
Biological Behavior
• Exhibits locally aggressive behavior with infiltrative growth
• No capacity for metastasis
TREATMENT (Fig. 6-12)
• Wide resection recommended
• Possible/low recurrence
• Excision with curettage alone has recurrence rate of 40%
• Addition of cryosurgery to a curettage may lower the recurrence rate
• Role of radiation and chemotherapy are unclear
• Amputation for multiply recurrent tumors or those that are unresectable
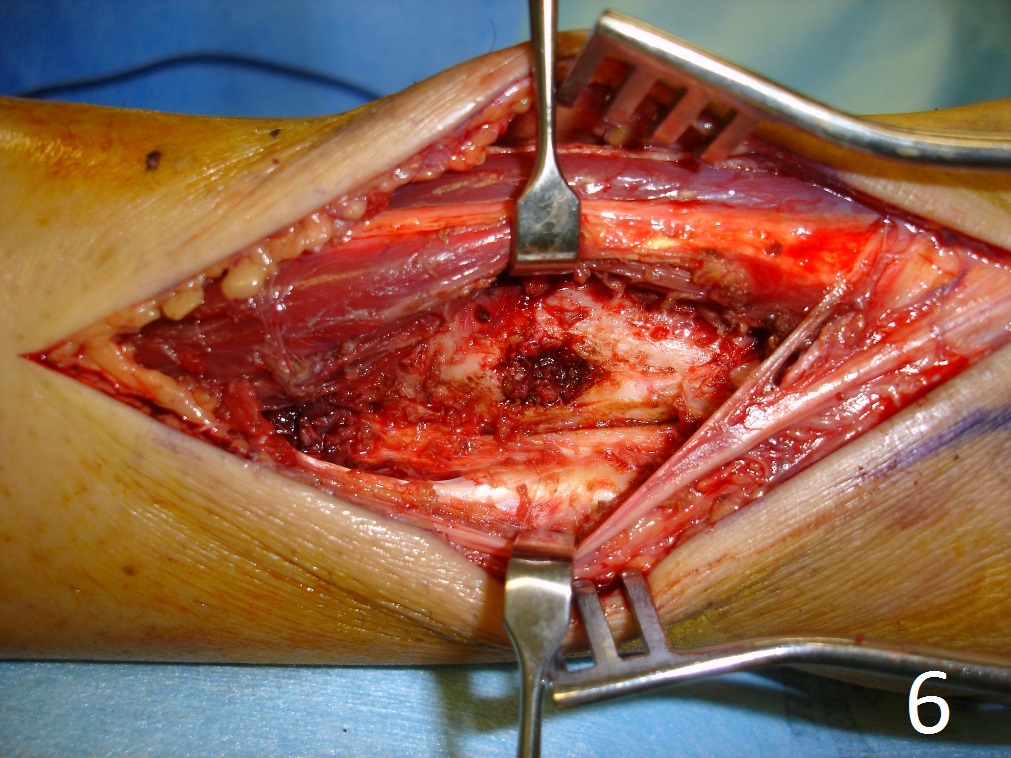
Fig. 6
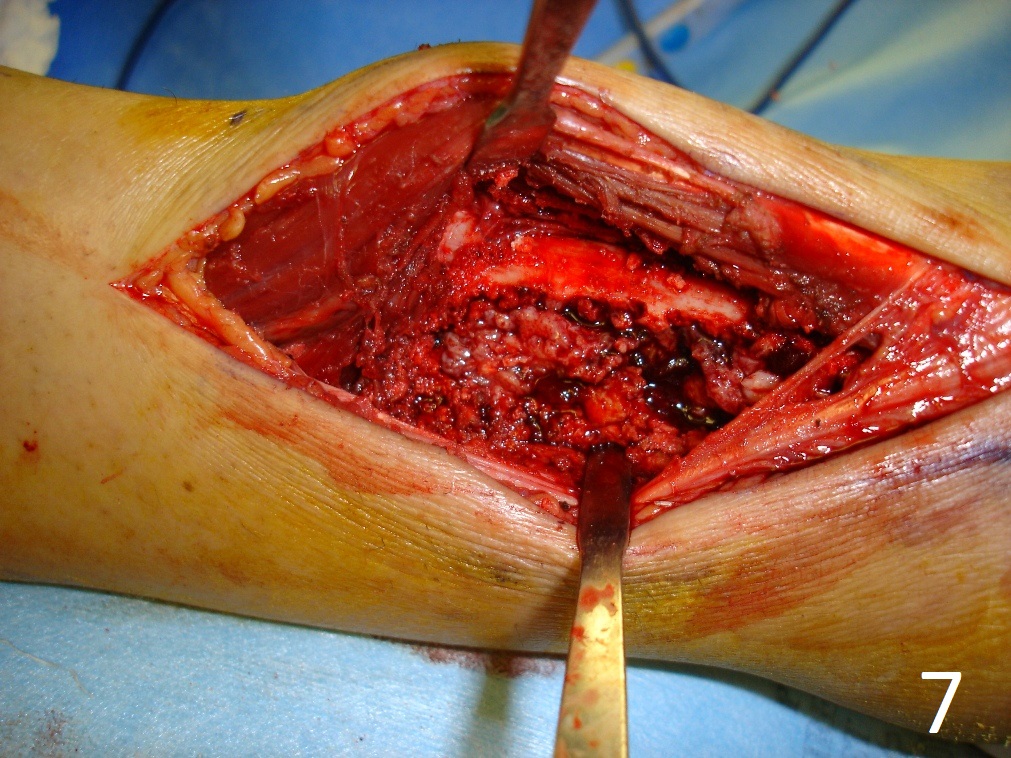
Fig. 7
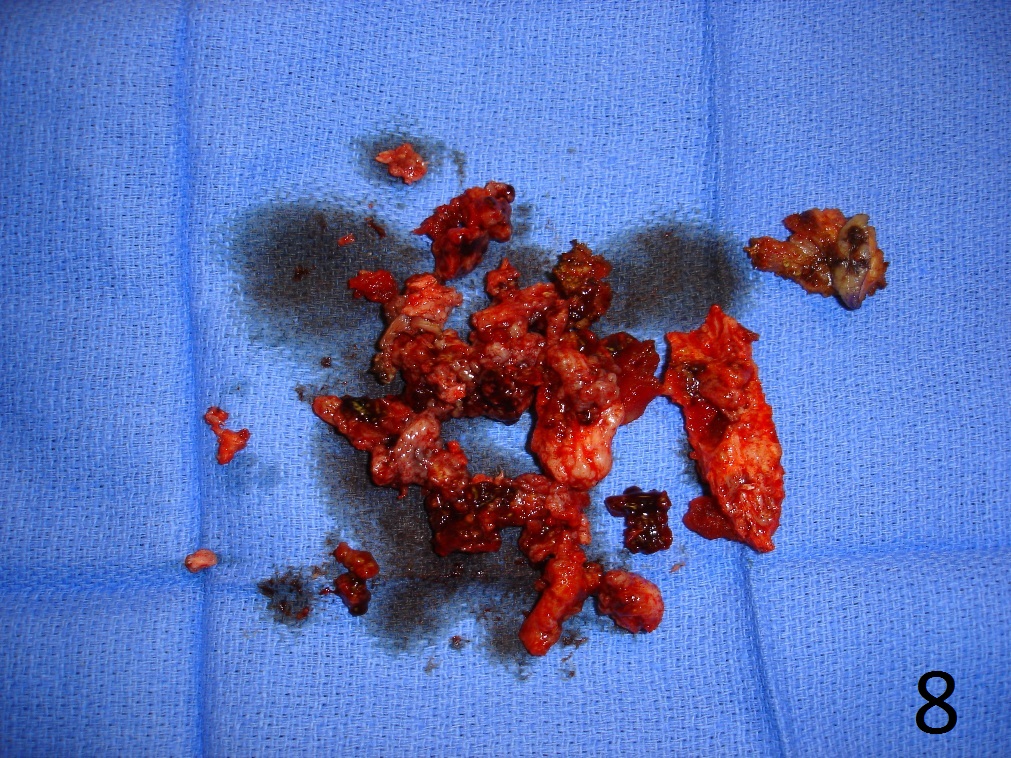
Fig. 8
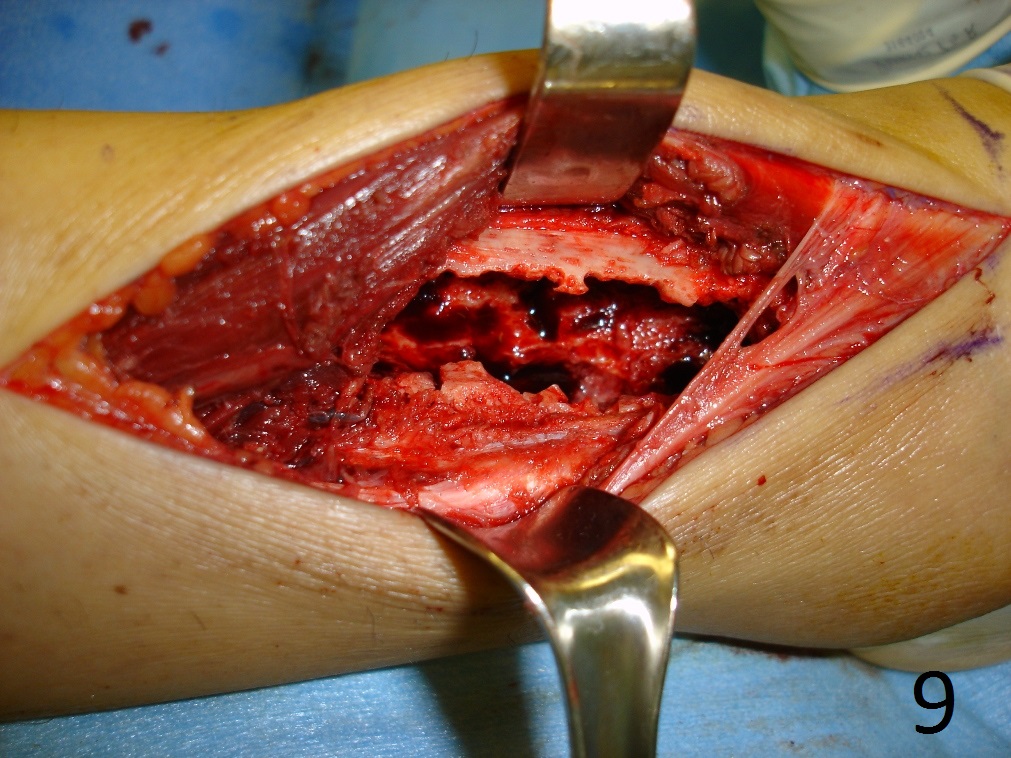
Fig. 9

Fig. 10
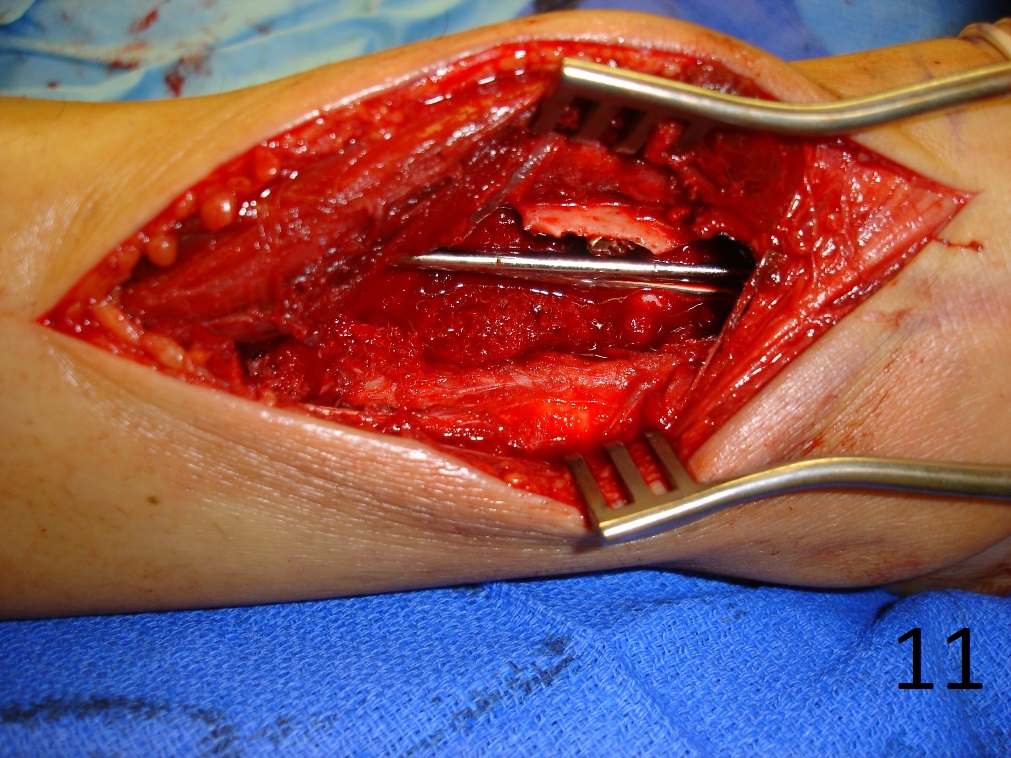
Fig. 11
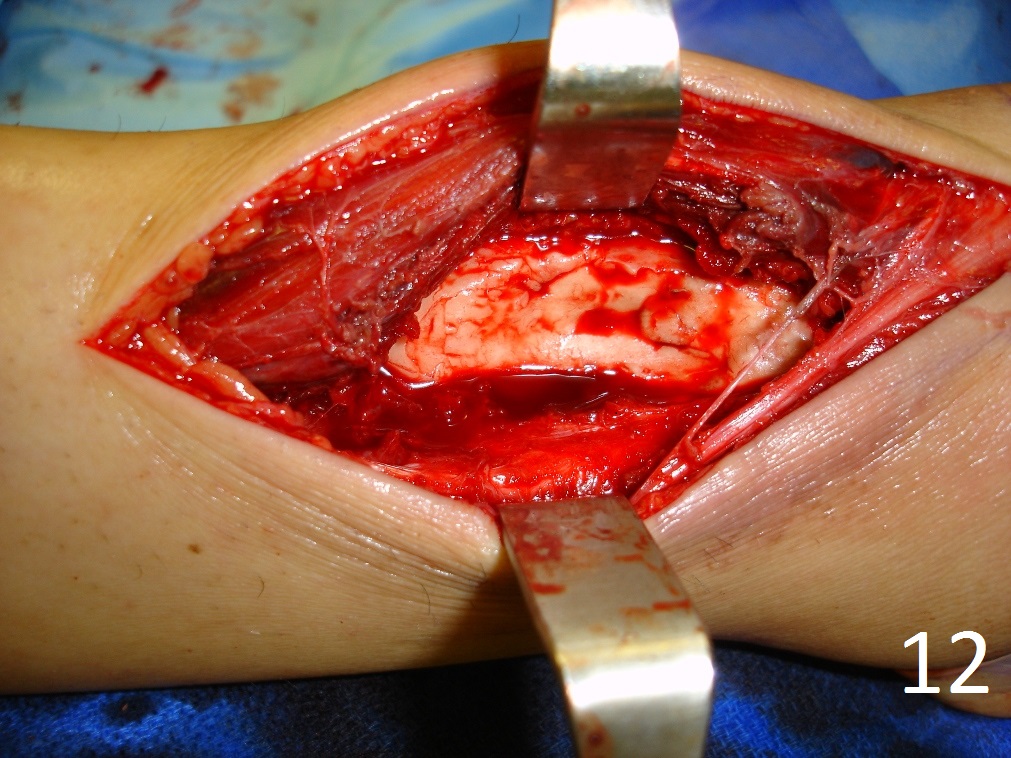
Fig. 12
Fig. 6-12: Intraoperative photograph of the lesion (Fig. 6) and steps of the treatment (Fig. 7-12), excision, cryosurgery, gross specimen and cemented internal fixation

Fig. 13: Postoperative image of distal tibia-fibula shows the fixation.
