GENERAL INFORMATION
Bone island, also called an enostosis, is a benign bone tumor mostly encountered as an incidental and asymptomatic finding. They are round and small (2 to 20 mm) intramedullary condensations composed of lamellar cortical bone. Essentially it is intramedullary displacement of compact lamellar bone. Any bone can be involved, but most common areas include the pelvis, ribs and proximal femur; affecting the epiphysis or metaphysis. Enostoses are diagnosed radiographically, and biopsies are usually not necessary. Differential diagnosis includes: sclerotic metastatic lesions, osteoid osteoma, sclerotic osteosarcoma, calcified enchondroma, bone infarct.
On radiographs, enostoses are round to oval and sclerotic lesions, without a periosteal reaction or bony destruction (Fig. 1). They have in the periphery of the lesion "feather-like spicules", resembling a "brush border" making this feature useful to recognize them. The spicules at the periphery blend in with the surrounding bony trabeculae. CT shows a blastic lesion, without periosteal reaction with radiating spicules at the periphery. The spicules may be more discernible on a CT scan than on plain x-ray (Fig. 2). MRI, shows no bone disruption or bony destruction, and is hypointense on both T1 and T2 weighted MR images. Bone islands are inert on bone scans, except when they are large. They may be quite active and hence may be worrisome for a malignancy.
Grossly, sharply circumscribed hard lesion in medullar canal with radiating spicules toward periphery. Microscopically, compact lamellar (cortical) bone with haversian systems surrounded by medullary bone (Fig. 3-4). No atypical nuclei or mitoses.
Does not require treatment. Patients should be observed. Follow-up for questionable lesions (large lesion can be confused with osteosarcomas). Radiographs and/or CT scans at 1, 3, 6, 12 months; if grows too rapidly.
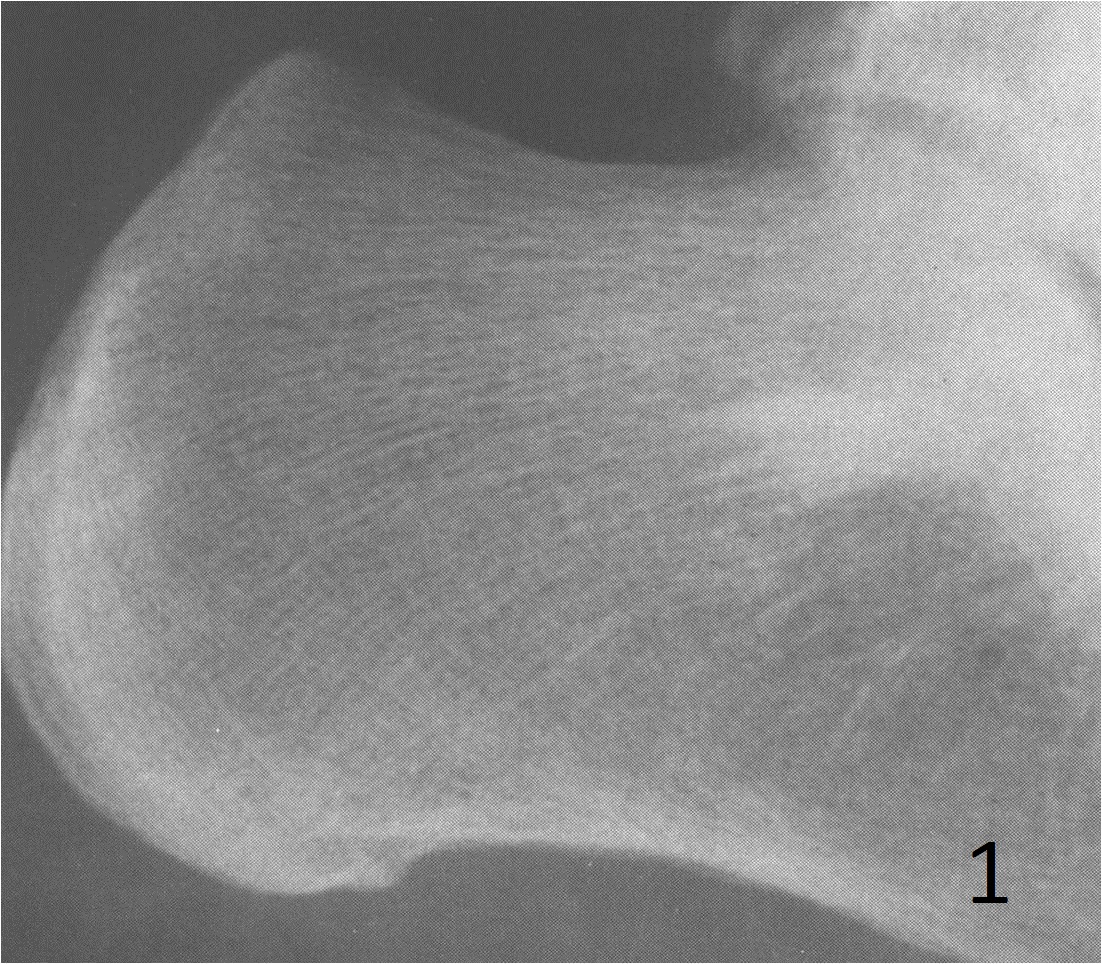
Fig. 1: Lateral plain Xray of calcaneous shows a bone island near the subtalar joint. The bone island appears as a sclerotic and spiculated lesion. This lesion was found incidentally during an evaluation for a sprained ankle.
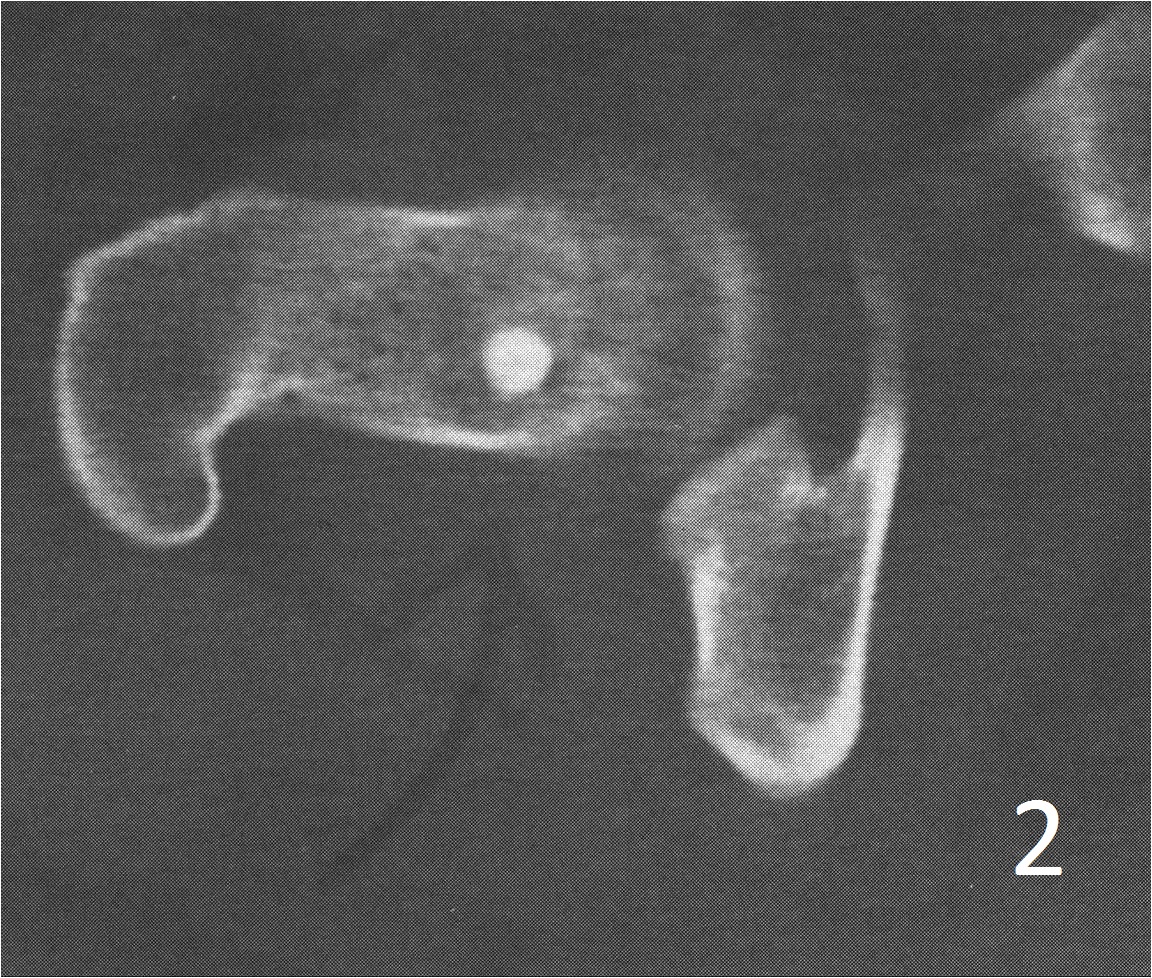
Fig. 2: Axial CT scan of the hip demonstrates a round blastic lesion in the femoral neck consistent with a bone island.
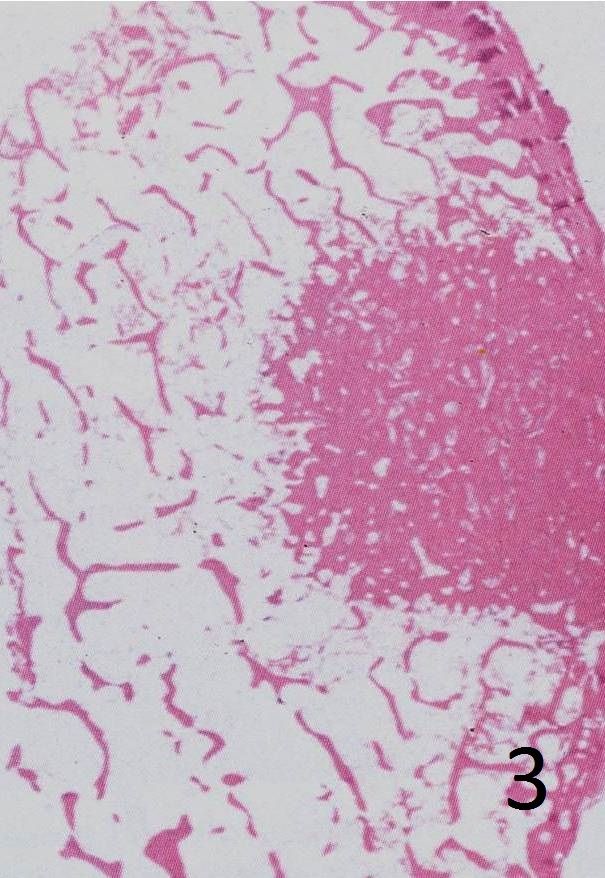
Fig. 3: Microscopy: Low power magnification of an enostosis shows a small well circumscribed sclerotic lesion made of compact lamellar (cortical) bone, surrounded by spongy cancellous bone. The trabeculae at the periphery of the bone island radiate outward as thorny spicules and blend with the normal trabeculae of cancellous medullary bone.
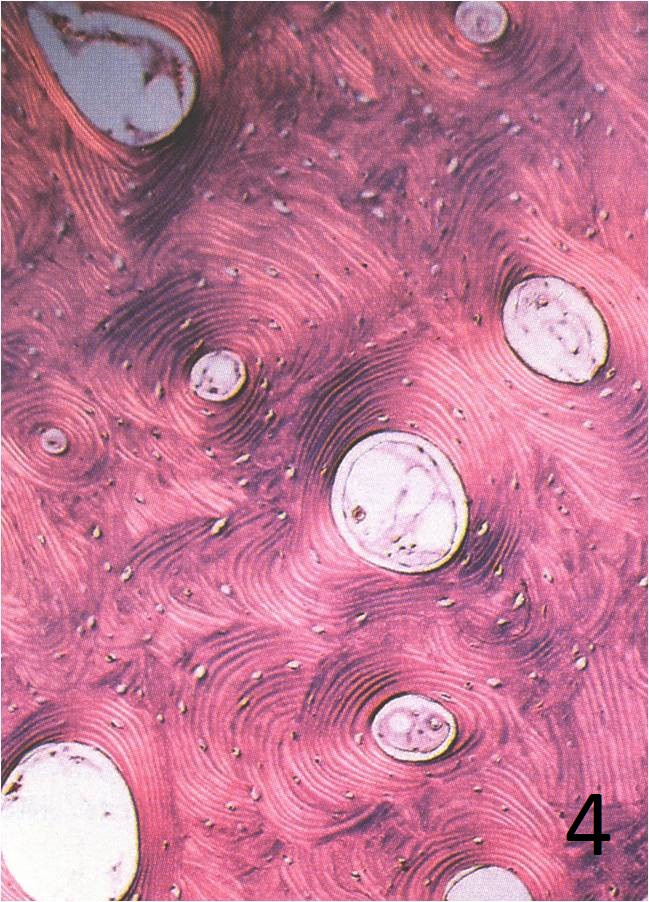
Fig. 4: Microscopy: High power magnification of an enostosis showing compact lamellar bone with haversian systems.
