GENERAL INFORMATION
Benign Fibrous Histiocytoma is a rare tumor of mesenchymal origin. First described in 1958 by Dahlin. They are composed of two cell types, namely atypical fibroblasts and histiocytes, arranged in a storiform pattern. Lipid-filled cells may be conspicuous and occasionally are the major component. These types of benign fibrous histiocytomas are known as xanthomas or fibroxanthomas. Benign Fibrous Histiocytomas are microscopically very similar to non-ossifying fibroma. It is essentially a non ossifying fibroma that grows in and unusual location or in an unusual age group. It can grow aggressively as opposed to a true NOF which is an indolent non aggressive growth.
CLINICAL DATA
• 1% of the benign bone tumors
•
More frequent in patients older than 20 years
•
Normally asymptomatic
•
Benign behavior
•
Metastases are rare.
Differential Diagnosis
• Non-ossifying fibroma
CLINICAL PRESENTATION
Signs/Symptoms
• Usually asymptomtic
• Localized pain
• Impending or pathologic fracture
Prevalence
• No race or sex predilection
• Very rare
Age
• All ages
• Adults more commonly affected, 20 to 50 years.
Sites
• One third arise around the knee (distal femur or proximal tibia)
• One third from the wing of the Ilium
• The rest arise from the ribs, fibula, skull, etc.
RADIOGRAPHIC PRESENTATION
Plain x-ray and CT scan
• Lytic lesion (Fig. 1, Fig. 2 & Fig. 3)
• Well-defined
• Geographic margins
• Eccentric
• Majority have well-defined sclerotic rims
• More aggressive lesions may have irregular margins
• Frequently produce endosteal erosion and cortical thinning
• Trabeculation may be seen
• In long bones, metaphysis, epiphysis, or diaphysis may be involved
MRI (Fig. 4-7)
•
Central low signal intensity with peripheral enhancement on T1-weighted images
• Heterogeneous high signal intensity with low signal in surrounding sclerotic bone on T2-weighted images
 Fig. 1
Fig. 1

Fig. 2
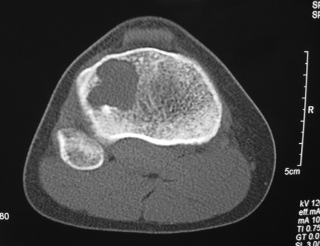
Fig. 3
Fig. 1-3: AP and Lateral plain x-rays of a benign fibrous histiocytoma shows an eccentric lytic lesion in the proximal tibia, well- demarcated with a prominent sclerotic rim. No soft tissue mass or trabeculations are seen.
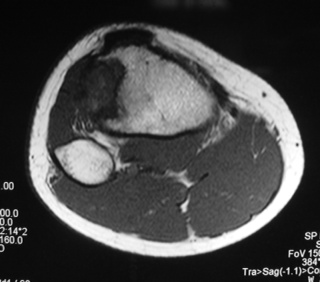
Fig. 4
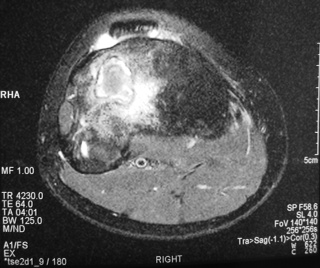
Fig. 5

Fig. 6

Fig. 7
Fig. 4-7: MR imaging of a benign fibrous histiocytoma of the proximal tibia demonstrates a heterogeneous high signal intensity and low signal intensity with surrounding sclerotic bone on T2-weighted images. T1-weighted images show low signal intensity. No soft tissue mass is visible.
PATHOLOGY
Gross (Fig. 8)
•
Dependent on amount of lipid, fibrous tissue, and hemorrhage
• May be gray, yellow, white, or red
• Soft or firm
Microscopic (Fig. 9)
•
Variable proportions
• Fibrous tissue
• Storiform pattern
• Multinucleated giant cells
• Foam cells
• Occasionally numerous
• No cytologic atypia
• Cholesterol clefts and hemisoderin deposits
• Mitotic figures occasional
• No atypical forms
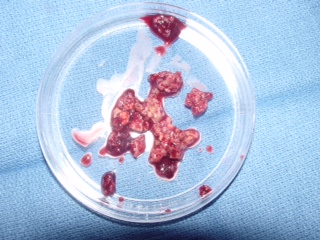
Fig. 8: Gross Pathology of a benign fibrous histiocytoma demonstrates multiple pieces of grayish fibrous tissue.
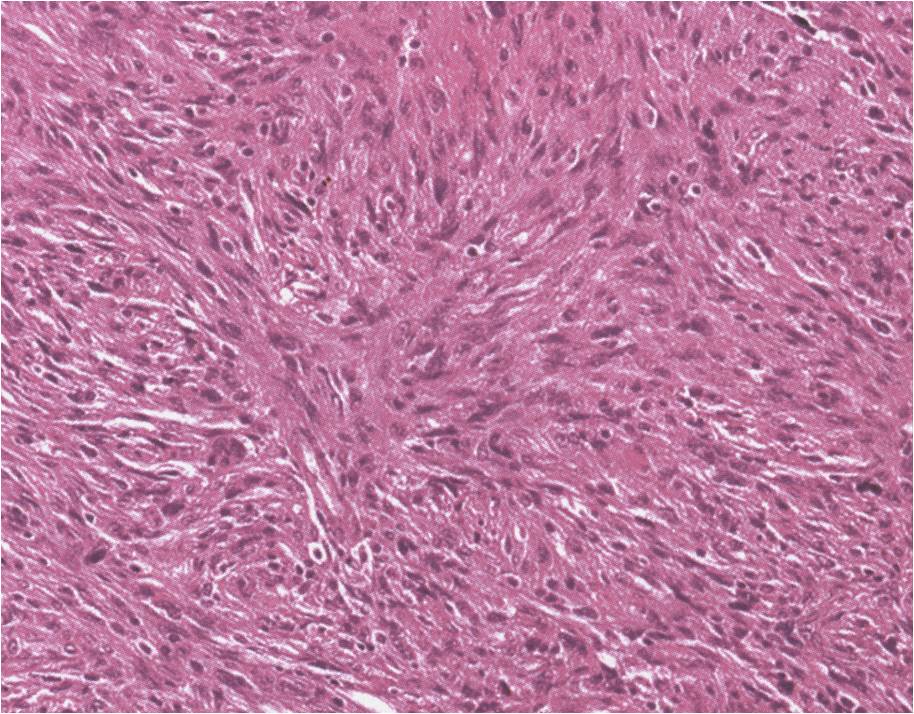
Fig. 9: Microscopic Pathology of a benign fibrous histiocytoma demonstrates abundant fibrous tissue in a storiform pattern distribution. No atypical forms or mitotic figures are distinguished. Lipid laden macrophages can be seen in a BFH (xanthoma cells)
PROGNOSIS
Biological Behavior
• Generally not aggressive
• Rare exceptions
• Moderate recurrence rate is between 5 to 25%.
• Generally depends on amount of lipid cells, greater lipid component is related with less recurrence rate.
• Metastasis are rare
TREATMENT
• Curettage (Fig. 10 & 11)
• Usually initial treatment
• Adjuvant therapy is recommended to reduce the recurrence rate. Cryotherapy for benign aggressive tumors has excellent results reducing the recurrence rate to approximately 3 to 5 %.
• En bloc excision may also be used if anatomic location allows for it and when multiple recurrences the lesion is unresectable.
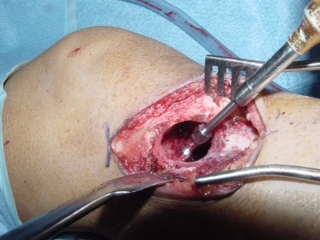
Fig. 10

Fig. 11
